Addiction Medicine

Often used to mask other diagnoses, addiction is a problem with the potential for serious consequences. Seasoned and credentialed professionals offer RCBM's outpatient addiction treatment services in a caring, confidential, and non-judgmental environment.
At the Rochester Center for Behavioral Medicine, we offer an innovative multidisciplinary treatment approach to recovery. Our program has been developed through years of experience working with clients who have multiple addictions. Recent discoveries in addiction science have expanded our understanding of addictions and their impact on the human brain. We have combined our years of experience with cutting-edge discoveries in neuroscience to provide highly effective treatment for our patients. We have dedicated clinicians who provide medication management along with individual psychotherapy by our certified advanced alcohol and drug counselors.
Do not wait for the legal system to make treatment mandatory. At RCBM, we encourage you to acknowledge responsibility and voluntarily seek treatment. Addictions are life-threatening concerns, and we are here to help.
What Substance Use Disorders We Treat
- Alcohol use disorder
- Opioid use disorder
- Prescription medication misuse
- Co-occurring disorders
Our Approach to Addiction Recovery
- Outpatient, evidence-based care
- Individual therapy
- Psychiatric support for co-occurring conditions
- Focus on relapse prevention and long-term wellness
What to Expect
- Initial assessment
- Collaborative treatment planning
- Ongoing counseling and medical management
- Coordination with external support if needed
FAQs
What is an addiction?
Continuing to use a harmful substance or engaging in destructive behavior despite knowing its consequences can have serious implications. Repeated abuse of substances can result in the pruning of neural pathways in the brain that are responsible for experiencing joy and happiness. Subsequently, your brain and body become accustomed to the repeated cycle of seeking a "high."
When you hear the word “addiction,” you may think solely of drug and alcohol dependency. However, substance abuse is not the only type of addiction. An addiction is formed whenever a habit turns into an obligation.
Process addiction refers to the compulsive urge to engage in certain behaviors or activities, such as gambling, internet use, or video games. It is a real condition that can have harmful consequences, just like substance addiction. While there are similarities between process addictions and substance abuse, there are also key differences in terms of symptoms, effects on the body, and treatment options.
Someone who frequently abuses substances may experience physical withdrawal symptoms, abnormal heart rate, psychotic episodes, or body pain due to the chemicals present in the substance they have consumed. or body aches due to the chemicals in the substance they have taken.
Process addiction is distinct from substance addiction as it does not affect the body in the same way. Since there are no chemicals involved, the symptoms of process addictions are behavioral in nature. Such symptoms include losing focus on work or school, damaging relationships due to a significant amount of time spent on the addiction, and a lack of desire or ability to do anything except engage in the process. Furthermore, process addiction can also cause an inability to focus on work or school and lead to a loss of relationships due to the time spent on the addiction. Other issues include the inability to focus on work or school, a loss of relationships due to time spent in the process, or a lack of desire or ability to do anything but their process.
Share Link: What is an addiction?
How do I know if I have a problem?
If you notice difficulty in your relationships, your work, or your finances, that may be a sign you have a substance use disorder. If you feel bothered by people telling you that you need to cut down or take risks to obtain a high reward, those are also signs that you need help.
Share Link: How do I know if I have a problem?
What are addictive substances and processes and how do they impact my body, mood, and my life?
Alcohol: Alcohol is also known as Ethanol, or ETOH, in medical terms. When alcohol is consumed, receptor sites in the brain are upregulated, acting like holes, asking to be filled with more alcohol. That is what causes a craving. When you consume alcohol, your brain releases a substance called GABA, or Gamma Amino Butyric Acid, which is your “keep calm” hormone. It also keeps your brain stable. When you drink alcohol, it releases GABA, making you feel calm. However, after such a large release, your brain is depleted, often leaving you feeling more anxious than when you started. When you add these aspects together, you can see how they lead to addiction. Over time, the constant depletion of GABA can lead to seizures.
Withdrawal: Withdrawal from ETOH can cause tremors, hallucinations, seizures, Delerium Tremens, coma, and death. The detoxification window for this is between 48 hours after stopping and up to 21 days after use ends. This is why alcohol detoxification must be done only with the guidance of a trained professional.
Benzodiazepines: Benzodiazepines are a class of drugs, also known as Z drugs. They contain Alprazolam, Lorazepam, Clonazepam, and Diazepam, among many others. They all have various uses and are best used in the short term. Patients get into trouble when prescribed an increasing amount when their initial dose’s effectiveness decreases over time. Benzodiazepines work by releasing GABA in the brain. GABA is the brain’s “keep calm” hormone and one of its main stabilizers. The constant use of Benzodiazepines in high doses depletes the brain’s GABA. This can cause seizures when they stop, especially if they stop abruptly. If a person has been at a certain dose over a period that exceeds what is safe, we will always recommend inpatient detoxification. A benzodiazepine withdrawal causes seizures, coma, and death. Safety is always the top priority.
Cannabis: Cannabis is perceived to be harmless because it produces neither overdose of fatal withdrawal. It is now legal and socially acceptable, making it even more unclear about its use. People all have an endocannabinoid system, the human body’s way of relieving pain and discomfort. Using cannabis affects our endocannabinoid system.
Cannabis is a drug that is classified as hallucinogenic. Although it does not cause hallucinations in everyone, it has the potential to do so under certain conditions. While it can provide temporary relief from hyperactivity and mania, the relief is short-lived and can lead to a larger rebound situation, prompting more cannabis use. When patients with bipolar disorder use it, they may experience temporary relief, but it can also lead to hallucinations, delusions, and paranoia, which is known as psychosis. This can also occur outside of a bipolar or schizophrenia diagnosis when used with stimulants. Stimulants can be either prescribed or obtained through caffeine, nicotine, or cocaine.
If you have a psychiatric diagnosis, avoidance of cannabis is the best policy.
Cocaine: Cocaine is another drug that mimics the effects of dopamine differently from opiates. It produces a feeling of power and euphoria in its users. The effects on the heart are notable immediately and over time, as it is extremely taxing on the heart muscle.
This drug is often used in patients who have undiagnosed ADHD, as it can provide energy, focus, and motivation during early use.
It is commonly abused by patients who suffer from bipolar disorder or major depressive disorder. In Bipolar patients, it can shift a patient from a depressive state into a manic state. In major depressive disorder, it can provide temporary relief from depression but rapidly leads to agitation and anxiety.
Kratom: Kratom is a plant that comes from parts of Asia. It behaves like an opioid in that 22 of the 35 chemical compounds attach to the Mu receptor in the brain. It is legal and available at smoke shops and gas stations. Many people have used it to attempt to come off opiates. It can cause typical opioid withdrawal syndrome and has been known to cause seizures upon withdrawal if usage has been lengthy or from a high dose. Use over time leads to insomnia and tremors.
Opiates: Opiates attach themselves to the Mu receptor site in the brain. They mimic the effects of your brain’s dopamine so closely that it signals your brain to stop making dopamine. Opiates, however, do not function in the brain the way native dopamine does, therefore the longer you take them, the more your own dopamine is depleted, setting you up for an increased need over time. Since dopamine is associated with joy, focus, and energy, the depletion of it over time causes physical pain, anxiety, and depression. Opiates lower your body’s drive to breathe. When a person overdoses, they stop breathing.
Long-Term Consequences of Opiate Use: Opioid Hyperalgesia is a condition that develops over time with regular use of opiates. It causes chronic aching pain in the joints and muscles around the body. It also causes poor focus, lack of energy, and brain fog. It is often confused with Fibromyalgia, which is a condition that produces similar sensations in the body and mind. When patients with Fibromyalgia are treated with opiates, Opioid Hyperalgesia often develops, worsening the condition. Opiates are not the correct treatment for fibromyalgia.
Withdrawal: Withdrawal from opiates is not fatal, but it can be a serious and intense experience. Symptoms of opiate detox may include a runny nose, yawning, pain, nausea, vomiting, diarrhea, restless legs, depression, agitation, and insomnia. The severity of these symptoms depends on the amount and duration of opiate use. Suboxone, a medication used to treat opiate addiction, has a longer half-life than heroin or painkillers, which can result in a longer post-acute withdrawal phase. This phase is characterized by symptoms such as poor focus, brain fog, restless legs, and insomnia due to the amount and duration of the substance used.
Psilocybin, LSD, DMT: These hallucinogenic drugs are often used in an attempt to reach greater peace, spirituality, or understanding of the universe. They can produce hallucinations because they affect the dopamine in the Optic Nerve, where your eyes and brain meet to process sight. Mushrooms are perceived as safe, because they are “natural,” but can affect the brain's ability to distinguish reality from dream states. This can lead to a variety of injuries or accidents.
The use of LSD or DMT can cause a permanent condition called HPPD, Hallucinogen Persisting Perception Disorder. This condition is permanent and causes hallucinations at various times without using the drug. It does not respond to anti-psychotic drugs the way hallucinations of Bipolar or Schizophrenia respond.
Gambling: Television now bombards people with options for online casino-style gaming. The legality and the availability of gambling make it a temptation for people who lack dopamine, as the thrill of winning elevates dopamine quickly.
Sex/Pornography Addiction: Those who are addicted to sex are often seeking a spike in dopamine. It is most seen in attention deficit hyperactivity disorder and bipolar disorder. ADHD is so highly stimulating that a person who lacks dopamine will be more prone to the rapid rise that sex or pornography can provide. In bipolar disorder, a manic state can produce feelings of hypersexuality.
Shopping:
Shopping addiction is a type of behavioral addiction that involves an uncontrollable urge to buy things as a way to feel better and avoid negative emotions like anxiety and depression. Like other behavioral addictions, shopping addiction can become an obsessive preoccupation that can cause problems in other areas of your life.
Share Link: What are addictive substances and processes and how do they impact my body, mood, and my life?
How we support co-occurring mental health and substance use challenges
Attention Deficit Hyperactivity Disorder (ADHD):
One of the most common triggers for alcohol abuse is ADHD. Undiagnosed and, therefore, untreated ADHD causes more than just inattention or hyperactivity for many patients; it can prime patients for addiction. ADHD is associated with a dopamine deficiency in the brain's pre-frontal cortex, where thinking, judgment, and decision-making reside. It is not just the brain’s stimulant but also the brain’s joy. Without it, your body compensates by releasing more Adrenaline, also known as the Fight or Flight Hormone. It can feel terrible, so a GABA (Gamma-Aminobutyric Acid) releaser like GABA often provides short-term comfort and long-term difficulty. GABA regulates nerve cell activity and has a calming effect on the central nervous system.
If you lack dopamine, you may crave “Dope.” If taking an opiate increases your level of energy, that may be an indication that you have undiagnosed ADHD. Many people do not realize that they are deficient in dopamine until they have surgery and experience an opiate. For these patients, at first, it may seem like a cure for anxiety, inattention, racing thoughts, and lack of energy. It is short-term relief with an excessively big rebound effect. That is how many people become addicted following an injury or surgery.
Bipolar Disorder:
Opiates often provide a sedating effect for patients with bipolar Opioids can have a sedating effect on bipolar disorder patients; however, they can cause similar complications as ADHD, as the artificial dopamine may deplete the natural dopamine.
Bipolar Disorder is also a risk factor for alcohol addiction. The highs and lows of bipolar also make people tend to gravitate toward a drug that releases GABA.
Generalized Anxiety Disorder:
This condition is partly caused by a deficiency of serotonin, also known as the calm, happy hormone. People who lack this chemical tend to be calmed by the immediate relief they feel upon the release of GABA. Still, the rebound of anxiety is so high that it becomes even more challenging to resist the urge when the anxiety returns.
Major Depressive Disorder:
This condition is also known as one partly driven by a lack of serotonin and other chemical mediators. It tends to provide instant relief of the pain of suffering by the temporary numbing effect it provides, yet it is the most powerful depressant drug available by legal purchase. The rebound effect of alcohol on depression is so severe that the constant pursuit of numbness becomes the goal.
Other Conditions:
Alcohol is often used as a form of self-medication for various conditions such as post-traumatic stress disorder, obsessive-compulsive disorder, schizophrenia, and schizoaffective disorders, which can cause individuals to seek to numb memories, ease compulsions, and hide hallucinations.
Additional Information:
Alcohol renders anti-psychotic drugs ineffective, and no anti-depressant can overpower its effects. Additionally, alcohol can worsen depression and trigger suicidal thoughts.
Share Link: How we support co-occurring mental health and substance use challenges
What to expect from outpatient addiction services at RCBM
The treatment for addiction is personalized for everyone based on their unique needs. The first step is to diagnose the underlying cause of addiction accurately. Diagnostic tests are essential for identifying the root causes of self-medicating. No one becomes addicted if they are happy, healthy, and whole. Treating the underlying diagnosis is crucial in preventing a relapse. However, some medications can help reduce cravings, regardless of the underlying psychiatric diagnosis. Treating the underlying diagnosis is critical to preventing relapse, but some medications work to help reduce cravings, which work irrespective of the underlying psychiatric diagnosis.
Inpatient or Outpatient Detoxification: This determination is always made on a case-by-case basis. If a person has ever had a seizure of any kind, they must detox at an inpatient facility. If a person has certain pre-existing health conditions or has been using a substance copiously or over an extended period, inpatient treatment may be necessary.
Acamprosate: This is used exclusively for alcohol abuse and works similarly to naltrexone
Antabuse: This drug is used for alcohol abuse. It produces a sickening effect when alcohol is consumed. Flushing, nausea, vomiting, and racing heart are all common effects when alcohol is consumed while on Antabuse. This acts as a deterrent for relapse.
Naltrexone: This is the oral alternative to vivitrol. It must be taken daily for the best results. It can be used for opiates or alcohol relapse prevention.
Suboxone: Suboxone is a drug that is used for the Stabilization of Opioid Addiction. It contains both buprenorphine and naltrexone. Buprenorphine is a long-acting opiate, and naltrexone is a blocker for opiates. When taken together, it can prevent a fatal opiate relapse by reducing cravings but blocking any feeling of being high. This enables patients to regain function in a situation where they do not feel ready for an opiate detox. At RCBM, we attempt to taper patients off this drug as quickly as possible to live an opiate-free life. Suboxone is highly useful to ease the symptoms of opiate withdrawal and is most accessible to come off when patients use it briefly. We also have extensive skills in tapering patients off suboxone who have been on it for extended periods.
Sublocade: Sublocade (buprenorphine) is prescribed to help individuals who are dependent on opioids and have been taking buccal or sublingual buprenorphine for at least seven days. This extended-release injection is classified as an opiate partial agonist. Buprenorphine works by mimicking the effects of opioid drugs, thereby preventing withdrawal symptoms when a person stops taking opioids.
Vivitrol: This is a once-monthly injection that goes into the hip. It blocks the effects of opiates and alcohol for 30 days. If you relapse, you will not get drunk or high. It reduces cravings by resting in the alcohol or opiate receptor sites, quieting the brain into thinking it has gotten what it is craving. It allows the brain to heal much faster than by sobriety alone. If a person uses enough of the substance they have been abusing, they can overcome it, but that is less common.
Talk Therapy: This is an essential piece of any recovery. Overcoming addiction requires patience, accountability, honesty, and self-respect. Talk therapy provides the skills to obtain and maintain sobriety.
Medical Nutrition Therapy: Medical Nutrition Therapy addresses the impact of alcohol and illicit drug use on the body's ability to absorb nutrients, which can lead to nutrient depletion. These substances also tend to suppress appetite, increasing the risk of severe dehydration and vitamin deficiencies. In addition, nutrition intervention can help stabilize mood and reduce cravings. Our registered dietitians can help you achieve an optimal diet to prevent these problems.
Share Link: What to expect from outpatient addiction services at RCBM
How effective is addiction treatment at RCBM?
Effective treatment for addiction is now available. Thanks to innovative discoveries in addiction science, treatment for addictive disorders has come a long way. At RCBM, we utilize cutting-edge treatment protocols for the benefit of our patients, making lasting recovery within reach!
Share Link: How effective is addiction treatment at RCBM?
How do I get started in the addiction program at RCBM?
If you are a current patient at RCBM, please contact our office at (248) 608-8800. If you are new to RCBM, you can initiate the admission process by completing a new patient registration form. Once you submit the form, we will match you with one of our qualified prescribers and therapists specializing in addiction treatment and one of our registered dietitians. Please note that individuals must be residents of Michigan and willing to visit the office if necessary. We are committed to helping you throughout your recovery journey and look forward to working with you.
Share Link: How do I get started in the addiction program at RCBM?
Watch: Expert Insights on Addiction Medicine

Addiction Treatment
Aliya Pasik, PA-C, Program Director, Addiction Recovery Clinic discusses the RCBM Addiction Medicine Program at RCBM and how we can help.
Addiction and Relapse Prevention During COVID-19
Whenever there's a time of high stress, the risk of relapse or the risk of escalating use is increased. Judy Redmond, MA, LPC, LLP, CAADC and Aliya Pasik, PA-C discuss relapse prevention during COVID-19.
Addiction, Signs and Recovery | with Aliya Pasik, MS, PA-C
Aliya Pasik, MS, PA-C, is the Program Director of the Addiction Recovery Center at the Rochester Center for Behavioral Medicine. Aliya addresses the many forms of addiction and substance abuse, particularly as it relates to the 50+ demographic. She describes underlying conditions that lead to self-medication such as ADHD, loneliness, anxiety, depression, and boredom. Alcohol abuse seems to be on the rise, especially during the Coronavirus pandemic. Aliya also discusses specific clinical programs that she is spearheading, describes certain signs that lead to substance abuse, and provides medical, cognitive, and holistic ways for patients and their families to have conversations that lead to recovery.
Book Review - The Sobriety Manual by Aliya Pasik, PA-C
In her new book, Aliya Pasik, PA-C, explains various types of addictions and their consequences in easy-to-understand terms, as she guides you on how to get the help you need. Don’t wait for the legal system to make treatment mandatory. Addictions are life-threatening concerns, and this new book, The Sobriety Manual: The essential tool for sobriety, health, and happiness, is your companion on your recovery journey. Read more here: https://www.rcbm.net/behavioral-medicine/the-sobriety-manual/
Relapse Prevention Treatment
Judy Redmond, LPC, LLP, CAADC explains common triggers for relapse and that thoughts and urges are a normal part of recovery. She discusses the importance of noticing and using tools for long term sobriety such as building self awareness, understanding triggers, and treating underlying mental health issues such as anxiety, depression and ADHD. Being part of a recovery community can offer support to stay on track for long term sobriety.
Therapy and Addiction Recovery
David Price, LPC, CAADC discusses therapy as a central and transformative role in supporting someone through addiction. He explains that therapy helps patients safely explore psychological, emotional and behavioral patterns that drive their substance use. David uses strategies including CBT that looks at patterns, triggers and thoughts; relapse prevention planning for high risk situations and urges to delay impulses; motivational interviewing and stages of change.
What to expect during outpatient addiction counseling
Lisa Robinson, MA, LPC, CAADC discusses the components of her addiction counseling sessions that include a comprehensive substance use and mental health history, building trust, identifying support systems, setting goals and objectives, along with steps to achieve goals and building coping skills.Meet the Providers Who Offer Care for Addiction Medicine

Joel L. Young, MD, Medical Director and Founder
Read More

Aliya Pasik, PA-C
Read More

Carol Rembor, PMHNP-BC
Read More

David Price, MA, LPC, CAADC
Read More

Jamie Clark, LMSW
Read More

Jennifer Stone, MA, LPC, NCC, CAADC
Read More

Judith C. Redmond, LPC, LLP, CAADC
Read More

Julie Staples MA, LPC NCC
Read More

Kendra Ball, LMSW
Read More

Lisa Mindell, LMSW
Read More

Lisa Robinson, MA, LPC, CAADC
Read More

Matthew Barsenas, LMSW, JD
Read More

Olivia Nash, MA, LPC, NCC
Read More

Sarah Krasnick, MSN, RN, ANP-C, PMHNP-BC
Read More

Taylor Drozd, LMSW
Read More
Related Titles from the RCBM Reading and App list:
Adult Children of Alcoholics - By Janet WoititzAdult Children of Alcoholics: Dysfunctional Families - By ACOA World Services
After the Tears: Helping Adult Children of Alcoholics Heal their childhood trauma - By Jane Middleton-Moz & Lorie Dwinell
Devastating Losses. How Parents cope with the death of a child to suicide or drugs - By William Feigelman, PhD
Smart Recovery Family and Friends Handbook For People Affected by the Addictive Behavior of a Loved One - By Smart Recovery
The Addiction Recovery Skills Workbook: Changing Addictive Behaviors Using CBT, Mindfulness, and Motivational Interviewing Techniques - By Suzette Glasner-Edwards PhD
When Your Adult Child Breaks Your Heart: Coping with Mental Illness, Substance Abuse, and the Problems That Tear Families Apart - By Joel Young, MD
ADHD Coaching

ADHD coaching can be an important part of a comprehensive treatment program for individuals with ADHD. ADHD coaches educate clients regarding this disorder. They reframe negative beliefs, identify individual learning styles, and develop systems and strategies to overcome strategies. Individuals with ADHD struggle with time management, organization, impulsivity, and procrastination. Coaching offers individualized and action-oriented approaches to combat these issues. Coaches are focused on developing productive habits and systems that lead to more productive lives. Several of our RCBM therapists have expertise in ADHD coaching.
Watch: Expert Insights on ADHD Coaching

What is ADHD Coaching?
Angela Eddy, MA, LPC, NCC describes the process of ADHD coaching whose purpose is to develop practical strategies for managing challenges related to executive functioning, time management organization and self-confidence.ADHD Medication Management

RCBM is dedicated to educating and helping individuals with attention-deficit/hyperactivity disorder, providing expert guidance for children, adolescents, and adults navigating this complex condition. How to find the right psychiatrist for ADHD and understanding the signs you may need therapy are critical steps toward effective management.
Joel Young, MD, Medical Director and Founder of RCBM, is a leading authority in ADHD treatment. He has authored several books and numerous articles on ADHD medication management, sharing insights on the latest advancements in care. His work emphasizes a comprehensive approach, blending medication, behavioral strategies, and therapy to help individuals succeed in school, work, and daily life.
What is ADHD?
Attention-deficit/hyperactivity disorder is a chronic condition that affects millions of children and often continues into adulthood. It presents as a combination of persistent symptoms, including:
● Difficulty sustaining attention
● Hyperactivity and restlessness
● Impulsivity and difficulty with self-regulation
How ADHD Affects Daily Life
ADHD can significantly impact academic performance, career progression, and personal relationships. Children with ADHD may struggle with low self-esteem, difficulty forming friendships, and challenges in school performance. Symptoms can persist into adulthood without proper treatment, affecting work productivity, financial management, and emotional well-being.
Many individuals wonder, "Do I need ADHD medication?" or "How do I know if therapy can help?" The proper treatment plan is personalized and may involve a combination of the following:
● Medication management for ADHD to help regulate focus and impulse control
● Behavioral therapy to develop coping strategies
● Executive function coaching to improve organization and time management
● Family support programs to help loved ones understand ADHD's impact
Finding the Right ADHD Specialist
If you are wondering how to find the right psychiatrist for ADHD, the team at RCBM provides individualized assessments to determine the best course of treatment. Our specialists help identify whether ADHD medication, therapy or a combination of both is the right approach based on a thorough evaluation.
If you or your child are experiencing signs you may need therapy for ADHD, such as persistent difficulty concentrating, frustration in school or work, or emotional dysregulation, we encourage you to schedule a consultation. Our team can help you understand whether ADHD medication or therapy is the right choice for you.
Watch: Expert Insights on ADHD Medication Management

ADHD Medication Isn’t Enough - What Else Can Help Your Child Focus?
Ashley Crowder, MA, LPC, discusses how to help your child stay focused when their ADHD medication does not last all day. This includes a schedule with routine along with unstructured time for creativity. Visual schedules including chore charts that can be checked off upon completion along with reward stickers that can lead to non-monetary awards.ADHD Treatment


RCBM is dedicated to educating and helping those who have ADHD. Joel Young, MD, Medical Director and Founder of RCBM, has authored several books and numerous articles on ADHD and is dedicated to helping those who struggle with this condition.
Attention-deficit/hyperactivity disorder (ADHD) is a chronic condition that affects millions of children and often continues into adulthood. ADHD includes a combination of persistent problems, such as difficulty sustaining attention, hyperactivity, and impulsive behavior.
Children with attention issues may also struggle with low self-esteem, troubled relationships, and poor performance in school. Symptoms sometimes lessen with age. However, some people never completely outgrow their ADHD symptoms. But they can learn strategies to be successful.
What is ADHD and Who Do We Help?
ADHD affects individuals across all age groups. At RCBM, we provide support for children, adolescents, and adults navigating challenges with focus, attention, impulsivity, and executive functioning.
Whether it’s a child struggling in school or an adult experiencing burnout and disorganization, our team is here to help.
Our ADHD Treatment Approach
- Our multi-disciplinary care model offers:
- Comprehensive psychiatric evaluations
- Individualized medication management
- Therapy and behavioral coaching
- Parent and school collaboration
Treatment plans are tailored to each patient’s needs, emphasizing long-term success and quality of life.
Why Choose RCBM for ADHD?
- 30+ years of experience treating ADHD across the lifespan
- Integrated care from psychiatrists, therapists, and ADHD coaches
- Compassionate support for families, schools, and individuals
Services We Offer
- ADHD diagnosis & treatment
- Executive functioning support
- ADHD coaching
- Medication management
- Family & school consultation
What to Expect
- Initial consultation and assessment
- Collaborative treatment planning
- Follow-up sessions and ongoing support
FAQs
What is ADHD?
ADHD is a common disorder, affecting between 6% and 10% of the American population. It is characterized by difficulties with attention, concentration, hyperactivity, and impulsivity. These symptoms often start in childhood and persist into adulthood. If you are experiencing any of these symptoms, RCBM can assist you in obtaining an accurate diagnosis. RCBM focuses significantly on identifying and treating attention deficit hyperactivity disorder (ADHD) at all stages of life. While it used to be known as ADD, it is now referred to as ADHD, which includes the hyperactivity component. ADHD is classified into three types:
- ADHD combined type
- ADHD predominantly inattentive type
- ADHD predominantly hyperactive-impulsive type
Share Link: What is ADHD?
What causes ADHD?
According to the National Institute of Mental Health, they include:
- Genetics (having a family member with the condition)
- Cigarette smoking, alcohol use, or drug use during pregnancy
- Exposure to environmental toxins during pregnancy
- Exposure to environmental toxins, such as high levels of lead, at a young age
- Low birth weight
- Brain injuries
Share Link: What causes ADHD?
How is ADHD diagnosed?
Everyone should be carefully evaluated. Our patients obtain a full diagnostic interview where we can understand the entire history and current concerns. In addition, psychological testing allows us to precisely diagnose the specific type of ADHD (ADHD combined type, ADHD predominantly inattentive type, ADHD predominantly hyperactive-impulsive type). Furthermore, we can diagnose other conditions that commonly co-occur with ADHD, which may include depression, anxiety, post-traumatic stress disorder (PTSD), panic disorder, learning disabilities, sleep disorders, and substance use disorders.
Furthermore, it's worth noting that many cases of chronic fatigue syndrome (CFS) are thought to be related to childhood ADHD. It's believed that brain fog and fatigue may be caused by similar biological processes involving dysregulation of the brain's dopamine and norepinephrine modulation. Some researchers have found that the presence of ADHD, along with CFS and depression, can amplify the intensity of fatigue and lead to an earlier onset of CFS.hly diagnosing ADHD in children, adolescents, and adults with ADHD through our psychological screening process.
Share Link: How is ADHD diagnosed?
What is the impact of ADHD on individuals diagnosed?
Studies reveal that adults with ADHD have difficulty throughout their lives with their job, schooling, interpersonal relationships, and overall well-being.ADHD has a direct impact on individuals and their families. Students with ADHD often face challenges in school, both academically and socially. They have high rates of school failure and often struggle with other mental health conditions. The difficulties associated with ADHD do not disappear in adulthood. Adults with ADHD frequently experience problems with distractibility, attention, and impulsivity. They are much more likely than the general population to suffer from anxiety and depression. Many report difficulties with insomnia or oversleeping. Studies show that adults with ADHD struggle throughout their lives with their job, education, interpersonal relationships, and overall well-being.
Share Link: What is the impact of ADHD on individuals diagnosed?
What is the treatment for ADHD?
Medication Management
Medication may also be part of the treatment plan for adults and children over 6. It can significantly improve focus. However, medication must not be skipped or missed, as symptoms may return.
Stimulants
Stimulants boost the brain chemicals dopamine and norepinephrine, which help you focus. Stimulants have been shown to improve symptoms in approximately 70 percent of adults with ADHD and 70 to 80 percent of children shortly after starting treatment.
Stimulants fall into three categories: short-acting (taken a few times a day), intermediate-acting (taken less often), and long-acting (taken once a day). Examples of stimulants include:
- Concerta, Ritalin, Daytrana, Jornay, Quillivant, Quillichew (methylphenidate)
- Adderall (amphetamine/dextroamphetamine)
- Evekeo (amphetamine sulfate)
- Vyvanse (lisdexamfetamine)
Non-stimulants also may be used but do not work as quickly as stimulants. However, they also help mitigate symptoms of ADHD by improving focus, attention, and impulsivity. Non-stimulants available for ADHD treatment include:
- Strattera (atomoxetine)
- Intuniv (guanfacine)
- Catapres (clonidine)
Antidepressants
Antidepressants may be used alone or in combination with stimulants to treat ADHD. They work similarly to stimulants, boosting the levels of dopamine and norepinephrine in the brain and improving both attention and impulsivity.
Psychotherapy
The American Academy of Pediatrics recommends behavior therapy for children six years old and under. This therapy teaches skills and strategies to help the child succeed at school, home, and in relationships. Behavior therapy for parents is also recommended for children of all ages.
It may also be recommended that children have a school treatment plan, including an Individualized Education Plan (or 504 plan) that describes the accommodations needed for the child, along with interventions and supports.
Accommodations may include:
- Receiving extra time on tests
- Receiving breaks or time to move
- Using technology to assist with tasks and additional help with organization
In recent years, cognitive-behavioral therapy (CBT) programs have been developed specifically for adults with ADHD. They can help overcome difficulties with executive functioning, improve time management and organization, and short-term and long-term planning.
Medical Nutrition Therapy
Diet is an integral part of ADHD management. Studies have shown that eating less processed food, sweets, and foods high in omega-3 fatty acids, such as fish, whole grains, fruits, vegetables, nuts, and seeds, can improve ADHD symptoms. In addition, certain foods may alleviate ADHD, while others may exacerbate it, so an individual nutrition plan is recommended.
Our registered dietitians will complete an assessment of your diet and develop a personalized nutrition plan to alleviate your symptoms. A thorough assessment paves the way for a successful nutrition counseling experience. At follow-up appointments, a review of food intake and behaviors, an evaluation of the meal plan, and further information are provided.
Share Link: What is the treatment for ADHD?
How effective is treatment for ADHD at RCBM?
RCBM has been actively involved in treating ADHD across the lifecycle for decades. The clinic has been involved in numerous clinical trials for ADHD medications. RCBM emphasizes diagnostic precision so that ADHD and co-existing conditions can be carefully understood and precise treatment applied.
Dr. Young has authored books and many articles on ADHD, and our treatment is cutting-edge.
ADHD Grown Up: A Guide to Adolescent and Adult ADHD
Contemporary Guide to Adult ADHD
Watch Dr. Young's interviews with local television stations:
ADHD in adults: Know the symptoms
What to know about national ADHD medication shortage
Share Link: How effective is treatment for ADHD at RCBM?
How do I get started with ADHD treatment at RCBM?
If you are a current patient at RCBM, don't hesitate to contact our office at (248) 608-8800. If you are new to RCBM, you can initiate the admission process by completing a new patient registration form. Once you submit the form, we will match you with one of our qualified prescribers and therapists specializing in ADHD treatment and one of our registered dietitians. Please note that individuals must be residents of Michigan and willing to visit the office if necessary. We are committed to helping you get the treatment you need and look forward to working with you.
Share Link: How do I get started with ADHD treatment at RCBM?
Watch: Expert Insights on ADHD Treatment
ADHD Medication Isn’t Enough - What Else Can Help Your Child Focus?
Ashley Crowder, MA, LPC, discusses how to help your child stay focused when their ADHD medication does not last all day. This includes a schedule with routine along with unstructured time for creativity. Visual schedules including chore charts that can be checked off upon completion along with reward stickers that can lead to non-monetary awards.
ADHD in the Workplace
Angela Eddy, MA, LPC, NCC, discusses common challenges adults with ADHD experience in the workplace. These challenges include organization, time management, focus, and communication. Angela suggests strategies for those who struggle, including planning tools, keeping a notepad handy, and maintaining a structured plan.
Coaching for ADHD
Angela Eddy, LPC, NCC explains how she structures ADHD coaching sessions including setting goals, tracking progress and building skills.
ADHD and Parenting
Angela Eddy, LPC, NCC explains how she works with parents to help their child succeed in managing their ADHD by focusing on progress, celebrating small wins, setting up predictable routines and scheduling their own compression time for self-care.
ADHD and Families
Angela Eddy, LPC, NCC gives advice for family members who struggle with ADHD. For example, by creating a menu of simple dinners for the week along with a running, joint shopping list, this can make evenings less stressful.
ADHD and Couples
Angela Eddy, LPC, NCC discusses how ADHD shows up in a marriage or long term relationship. She illustrates how to recognize ADHD in your partner to understand that their brain manages time, attention and emotions differently. With awareness and supports, couples can reduce conflicts and feel more connected.Related Titles from the RCBM Reading and App list:
10 Simple Solutions to Adult ADD - By Stephanie Moulton SarkisADHD Advantage - By Dale Archer, MD
ADHD Grown Up: A Guide to Adolescent and Adult ADHD - By Joel Young, MD
Contemporary Guide to Adult ADHD - By Joel Young, MD
How to ADHD - By Jessica McCabe
How to Keep House While Drowning A Gentle Approach to Cleaning and Organizing - By KC Davis
You Mean I’m Not Lazy, Stupid, or Crazy!? The Classic Self-Help Book for Adults with Attention Deficit Disorder - By Kate Kelly and Peggy Ramundo
Chipolo – tool for tracking/finding easy-to-lose items like keys, coffee mugs
Class Manager
ClearFocus
Focus keeper – pomodoro technique tool (Apply/iOS only)
MotivAider- Interval timer for self-monitoring; can be set to sound or vibrate options
PrioritizeMe
The HW App
Anxiety Disorder Treatment

Individuals with anxiety disorders can have worry and fear that are constant, overwhelming, and, at times, disabling. Symptoms associated with anxiety disorders can hinder an individual’s normal functioning. Treatments often alleviate symptoms, allowing significantly improved quality of life.
FAQs
What are the different types of anxiety disorders?
Agoraphobia
This is a specific type of panic disorder that occurs when an individual is in fear of being in places that would be difficult to escape, such as grocery stores, a car, crowds, open or closed spaces, etc.
Generalized Anxiety Disorder
Generalized Anxiety Disorder (GAD) is characterized by persistent and excessive worry about many aspects of life. Individuals may struggle to control their worry, leading to difficulty concentrating or general functioning.
Obsessive-Compulsive Disorder
Obsessive-Compulsive Disorder (OCD) is an anxiety disorder that involves both obsessions (thoughts, images, or impulses that occur repeatedly) and compulsions (acts that a person repeatedly performs to make the obsession go away). The brain seems to get “stuck” on a thought or urge it cannot move past. Individuals with OCD often have the sense that if that “obsession” continues without them taking part in any compulsions, the anxiety will become intolerable.
Panic Disorder
Panic Disorder is a fight or flight response to anxiety, which can trigger intense reactions to perceived danger or threat. Panic attacks can be very frightening because the individual usually loses control of their body. It may feel like the person is having a heart attack, trouble breathing, and, in some cases, even feel like the individual is dying. A lot of people experience a panic attack in their lifetime, usually not having a repetitive occurrence. Panic attacks become Panic Disorders when stressful situations or trigger events ensue recurrent panic attacks. When they begin to happen frequently, it can affect the quality of life of the individual who fears their next panic attack.
Performance Anxiety
Performance anxiety is a common issue that many people face when they are required to perform in front of others, whether it's in a work setting, on stage, or during a public speaking engagement. The fear of being judged or making a mistake can lead to physical symptoms such as sweating, trembling, or a racing heartbeat. It can also lead to mental and emotional distress, causing individuals to doubt their abilities and worry excessively about their performance. While a certain level of anxiety can be expected, severe performance anxiety can be debilitating and impact one's overall well-being.
Post-Traumatic Stress Disorder
Post-traumatic stress disorder (PTSD) is an anxiety disorder that occurs after a person has personally experienced or witnessed a dangerous and life-threatening event. Individuals who are at risk for developing PTSD include but are not limited to: Soldiers who have been in combat, survivors or witnesses of violent crimes (including rape, kidnapping, robbery, etc.), individuals who have lived through a natural disaster, survivors of accidents or grave illness. Re-experiencing symptoms, sometimes known as “flashbacks,” make the individual relive the trauma over and over. This could include physical symptoms like a racing heart, sweating, bad dreams, or frightening thoughts. Sometimes, the individual uses coping mechanisms, also considered avoidance symptoms, such as staying away from places, events, or objects that are reminders or triggers of the experience. Other symptoms of PTSD include feeling emotionally numb, feeling intense guilt, depression, or worry. Some individuals lose interest in activities that were once enjoyable and also have trouble remembering the traumatic event.
Separation Anxiety
Symptoms of separation anxiety may include recurrent and excessive distress about anticipating or being away from home or loved ones. Children are especially prone to separation anxiety during times of stress and tend to become excessively anxious when separated from their parents.
Separation anxiety differs from normal clinginess. Separation anxiety disorder is diagnosed when symptoms are excessive for the developmental age and cause significant distress in daily functioning. Children with the disorder cannot think about anything but the present fear of separation. They may have nightmares or regular physical complaints. They may be reluctant to go to school or other places.
School Anxiety Issues
Along with Social Anxiety, some children suffer from school-related anxiety issues. This could start with symptoms such as a headache, stomachache, or nausea before school begins. Sometimes, these symptoms can even lead to school avoidance due to the severity of the anxiety. School Anxiety can stem from the general fear of school and the concern of not having parents with them.
Social Phobia
Social Phobia, also known as Social Anxiety Disorder, is characterized by marked and persistent fear of situations in which one must perform or interact socially with or in front of others. A person with social phobia fears situations where they are exposed to new situations or people. They, therefore, worry about behaving in a way that others might judge them as foolish, unacceptable, inappropriate, or inadequate. When a socially phobic individual is exposed to these situations, they feel anxious, both physiologically and emotionally. This disorder hurts the individual’s social, academic, and occupational functioning.
Specific phobias
A specific phobia is any form of anxiety disorder that amounts to an unreasonable or irrational fear related to exposure to particular objects or situations. As a result, the affected person tends to avoid contact with the objects or situations and, in severe cases, any mention or depiction of them.
Trichotillomania
Trichotillomania is a disorder characterized by the pulling of hair for non-cosmetic purposes, which can often result in significant hair loss. Hair is typically pulled from eyebrows, eyelashes, scalp, beard, and pubic area, though hair from other parts of the body may also be pulled.
Share Link: What are the different types of anxiety disorders?
What are the causes of anxiety disorders?
Some individuals may experience anxiety as a result of an underlying health issue. In certain instances, signs and symptoms of anxiety could be the initial indicators of a medical condition. Medical problems that can be linked to anxiety include:
- Chronic obstructive pulmonary disease (COPD) and asthma
- Chronic pain
- Diabetes
- Drug or alcohol use
- Heart disease
- Hyperthyroidism
- Withdrawal from alcohol, anti-anxiety medications, such as benzodiazepines, or other medications
Other risk factors may include alcohol or drug use, a family history of anxiety, a history of trauma, certain personality traits, other mental health disorders, or stress.
Share Link: What are the causes of anxiety disorders?
How are anxiety disorders diagnosed?
RCBM is committed to accurately and thoroughly diagnosing anxiety disorders in individuals of all ages through our psychological screening process. All patients undergo a comprehensive diagnostic interview to understand their history and current concerns. Additionally, psychological testing helps us pinpoint the specific type of anxiety disorder along with co-occurring disorders.
Share Link: How are anxiety disorders diagnosed?
How are anxiety disorders treated at RCBM?
CBT
The Rochester Center for Behavioral Medicine uses Cognitive Behavioral Therapy (CBT) for the treatment of anxiety and depressive disorders. This therapy combines behavioral exposure therapy and cognitive restructuring to help the patient confront avoidance, correct negative automatic thoughts, and return to optimal functioning.
Mindfulness-based therapies
Mindfulness-Based Cognitive Therapy (MBCT) combines mindfulness-based stress reduction techniques such as yoga or meditation with traditional CBT. Several studies have demonstrated that MBCT can effectively alleviate anxiety, and there is also evidence suggesting that it can be an effective treatment for depression. In addition, deep breathing, relaxation, and visualization are also helpful adjuncts in managing anxiety.
Acceptance and commitment therapy (ACT)
ACT builds on CBT principles and operates on the theory that trying to avoid anxiety can keep you feeling anxious. ACT can help you learn new ways to acknowledge and address complex thoughts and feelings as they arise. Studies show that ACT can be an effective treatment for anxiety.
Treatment for PTSD
At the Rochester Center for Behavioral Medicine, PTSD is treated with a combination of cognitive-behavioral therapy and, when necessary, medications. This practical approach can help individuals with PTSD identify situations that trigger their “fight or flight” response. Using the cognitive-behavioral techniques of flooding and systematic desensitization, the therapist and patient can work together to safely reintroduce situations that have become too anxiety-provoking for the patient. Over time, irritability, flashbacks, and nightmares subside, the patient can return to their pre-trauma functionality, and long-term success is within reach.
Medication management
Medications can help alleviate the symptoms and improve functioning. Common medications for anxiety disorders include:
Antidepressants: While antidepressants are primarily used to treat depression, they can also be beneficial for managing anxiety disorders. These medications work by regulating the brain's use of certain chemicals to enhance mood and alleviate stress. It's important to note that antidepressants may take some time to take effect, so it's essential to be patient. The most commonly prescribed types of antidepressants for anxiety are SSRIs and SNRIs. Tricyclic antidepressants are another option, but they tend to have more side effects.
Benzodiazepines: These types of medications can reduce feelings of anxiety, panic, and worry. They work quickly, but you can become tolerant of them over time. They also have the potential for addiction, so you should use them with caution. Your healthcare provider might prescribe a benzodiazepine for the short term and then gradually reduce your dosage. Some benzodiazepines that can help with anxiety disorders are alprazolam, clonazepam, diazepam, and lorazepam.
Beta-blockers: These medications can help reduce some of the physical symptoms of anxiety disorders, such as rapid heartbeat, shaking, and trembling, but they do not address the psychological aspects of anxiety disorders.
Medical Nutrition Therapy
Nutrition intervention is an essential adjunct to the treatment of anxiety. A variety of foods from all food groups provide important nutrients and maintain stable blood sugar levels, which is crucial in managing anxiety. Our registered dietitians can develop a personalized nutrition plan to help with the management of anxiety.
Higher level of care treatment
An inpatient stay is recommended for individuals who are unable to care for themselves or may be a risk to the safety and well-being of themselves or others.
This might include individuals who are:
- Actively suicidal
- Actively homicidal
- Flagrantly psychotic
- Depressed or anxious to the point that the patient cannot engage in activities of daily living
Partial Hospitalization Program (PHP)
- This level of care is recommended for individuals who:
- Exhibit psychiatric severe or co-occurring disorders
- Present a danger to themselves or others
- Have not had success using outpatient treatment
This level of care is necessary to provide structure for treating current symptoms that cannot be managed at a lower level of care when current intensive outpatient care has failed to improve functioning or acute coping skill deficits are severe and require daily assessment and intervention.
Share Link: How are anxiety disorders treated at RCBM?
How effective is treatment for anxiety disorders at RCBM?
CBT is particularly effective for the anxiety disorder spectrum, such as panic disorder, post-traumatic stress disorder, obsessive-compulsive disorder, social anxiety disorder, and specific phobias. The hallmark of CBT is the patient’s role in learning and practicing skills outside the session to maximize the therapeutic benefit of this therapy. In mood disorders, the patient will learn coping skills to master tasks often thought too arduous for the depressed patient. The use of CBT with medication management is addressed, and the ultimate decision is made between the patient and the RCBM professional.
Using the cognitive-behavioral techniques of flooding and systematic desensitization, the therapist and patient can work together to safely reintroduce situations that have become too anxiety-provoking for the patient. Over time, irritability, flashbacks, and nightmares subside, the patient can return to their pre-trauma functionality, and long-term success is within reach.
Continue to work with your healthcare provider to determine the best medication combination and dosage for you. Do not adjust the dosage or discontinue medications without consulting your provider first. Your prescriber will monitor your progress to ensure the medicines are effective and do not cause any adverse side effects.
Medical nutrition therapy is also an essential intervention that works together with psychotherapy. Complex carbohydrates such as brown rice, oats, whole wheat, beans, and legumes can help increase serotonin levels in the brain, promoting peace and well-being. In addition, probiotics are helpful, as recent research shows a correlation between the lack of beneficial bacteria and microbes in your gut, resulting in anxiety. Our registered dietitians can help you include foods to manage your gut as an adjunct to treating your anxiety.
Share Link: How effective is treatment for anxiety disorders at RCBM?
How do I get started with treatment for anxiety disorders at RCBM?
If you are a current patient at RCBM, don't hesitate to contact our office at (248) 608-8800. If you are new to RCBM, you can initiate the admission process by completing a new patient registration form. Once you submit the form, we will match you with one of our qualified clinicians who specializes in treating anxiety disorders. Please note that individuals must be residents of Michigan. We are committed to helping you, or your loved one live a quality life and look forward to working with you.
Share Link: How do I get started with treatment for anxiety disorders at RCBM?
Watch: Expert Insights on Anxiety Disorder Treatment

Performance Anxiety
Nancy Tedder, MA, LPC discusses performance anxiety and how she can help those who are struggling.
What is Generalized Anxiety Disorder?
Matthew Barsenas, LMSW gives us an overview of generalized anxiety disorder (GAD), defining the mental and physical components of GAD, along with treatment.
What is Exposure and Response Prevention (ERP)
ERP is the gold standard for treatment of obsessive compulsive disorder (OCD). Alex Siegel, LLP explains that in ERP, the patient will learn how to confront obsessions while withholding from engaging in their compulsions, through a collaborative effort between the patient and the therapist.
What is Cognitive Behavioral Therapy (CBT)?
Dr. Melissa Oleshansky, PhD discusses cognitive behavioral therapy (CBT). This structured and goal-oriented psychotherapy is used at RCBM to treat or manage mental health conditions, stress, unhealthy habits, and emotional concerns.
College Mental Health
Melissa Oleshansky, PhD, gives advice on how to protect your mental health at college. She cautions against confusing overachievement with wellbeing as saying yes to everything can leave you depleted. Know when to slow down, create space to think and feel, build in daily movement and fresh air, or call someone. Reach out early - asking for help from a therapist, friend or family is not weakness, its emotional intelligence. You are worth taking care of.
When Mental Health Symptoms Warrant Urgent Care - But Not the ER
Jennifer Stone, LPC, NCC, CAADC discusses when to go to the emergency room for treatment vs urgent care. If you are an immediate risk to yourself including self-harm behaviors or suicidal thoughts, and/or the thought of doing harm to others, an ER visit is warranted. An urgent care visit would be warranted for non life threatening symptoms that impact daily living such as depression, anxiety, panic attack or sleep disturbances. In this situation, stabilization can take place with referral to a professional, such as RCBM clinicians, for long term management.Related Titles from the RCBM Reading and App list:
The Anxiety and Phobia Workbook - By Edmund BourneOvercoming Unwanted Intrusive Thoughts: A CBT-Based Guide to Getting Over Frightening, Obsessive, or Disturbing Thoughts - By Sally Winston and Martin Seif
The OCD Workbook: Your Guide to Breaking Free from Obsessive Compulsive Disorder - By Bruce Hyman and Cherry Pedrick
Autism Spectrum Disorder

Autism Spectrum Disorder (ASD) is the name for a group of developmental disorders. ASD includes a wide range, “a spectrum,” of symptoms, skills, and levels of disability. People with autism (ASD) often have some of these characteristics: ongoing social impairments such as difficulty communicating and interacting with others, repetitive behaviors, oversensitivity to sensory stimulation (tactile, sound, smells, taste, bright lights), and restricted range of interests or activities. These symptoms are typically recognized in the first two years of life. These symptoms impact the individual’s ability to function at school or work, family functions, or other areas of life.
Autism is a spectrum disorder with symptoms ranging from mild to severe. Treatments and services, including early intervention, can improve behavioral, developmental, educational, and social/emotional functioning. According to the Centers for Disease Control and Prevention (CDC), around 1 in 36 children has been identified with some form of autism.
FAQs
What is Autism Spectrum Disorder (ASD)?
Autism Spectrum Disorder (ASD) is the name for a group of developmental disorders. ASD includes a wide range, “a spectrum,” of symptoms, skills, and ability levels. Individuals with Autism (ASD) are neurodivergent, meaning their brain perceives the world and processes stimuli differently. This is typically exhibited through deficits or impairments in social interactions and communication and repetitive or restrictive behaviors. ASD differs for each person, thus emphasizing its “spectrum” of characteristics.
Share Link: What is Autism Spectrum Disorder (ASD)?
How is ASD diagnosed?
At RCBM, our screening and comprehensive psychological evaluation programs serve distinct but complementary roles in the diagnostic process. Diagnostic screening is always the first step—a targeted assessment to identify symptoms, guide accurate mental health diagnoses, and support a treatment plan. If the clinician believes the screening results may indicate ASD and a formal medical diagnosis is warranted, a referral for a comprehensive ASD evaluation will be made. Often, a diagnosis includes a level specifier to indicate the severity and required support. Typically, a formal diagnosis is not made before age 2 as many traditional behaviors of ASD are developmentally appropriate before 24 months of age.
The following components of the evaluation are individualized based on the referral.
Intake
- One hour
- Conducted virtually
- It will be discussed if additional tests, record reviews, or interpretations are required based on the referral.
Evaluation
- Approximately two-three hours
- In-person at our office
Feedback
- Scheduled three to five weeks after completion of the evaluation to review the findings and recommendations
- The time required varies depending on the referral concerns and individual needs.
Cost: While the intake and feedback sessions are billable to insurance companies, the in-person evaluation component is not billable to any insurer. The cost of the evaluation will be determined upon referral or completion of the interest form.
Please complete the interest form for comprehensive psychological testing, which includes evaluations for autism spectrum disorder along with specific learning disorders, accommodation testing, guardianship evaluations, and other related services. The evaluation is done in person.
Share Link: How is ASD diagnosed?
What are the symptoms of ASD?
It is important to note that no two individuals present with the same experience or symptoms. Behaviors also depend on an individual’s age, gender, and developmental stage. While the list below is not exhaustive, some common behaviors might include:
Ongoing social problems and difficulty communicating or interacting with others
- Not engaging in reciprocal conversation
- Lack of social play or joint attention
- Difficulty understanding social cues or maintaining eye contact
- Limited language or nonverbal
Repetitive behaviors
- Hand flapping, rocking, swaying, tip-toe walking
- Repetition of the same word or phrase
- Continually lining up objects or toys
Sensory issues
- Preferred food textures
- Discomfort with certain clothing materials or tags
- Overstimulated by loud noises or physical touch
Limited or fixated interests or activities
- Limited/restricted diet (May be sensory/texture-related)
- Speaking inclusively about a specific topic or interest
Difficulty or inflexibility with coping, change, or transitions
- Difficulty transitioning from one activity to another
- Emotional dysregulation occurs if things do not go as planned
- Inability to cope with sensory overload
- Poor frustration tolerance that may result in aggression or self-harm
- Cognitive perseveration stemming from some anxiety or worry
- Delayed processing and response time
Share Link: What are the symptoms of ASD?
What is the treatment for ASD and what type of support is available?
While ASD is not curable, several treatments and supports can improve behaviors and quality of life. RCBM offers psychotherapy, medication management, and medical nutrition therapy. Additional treatment options and approaches include occupational therapy, feeding therapy, speech therapy, and social/recreational autism-friendly events such as support groups, camps, and adaptive services. Another prominent evidence-based treatment for ASD is Applied Behavioral Analysis (ABA). RCBM does not offer this treatment but can help identify agencies that do and may be covered under insurance.
An essential first step after an ASD diagnosis is education. Our therapists will help explain and orient our patients and/or their parents to understand ASD better and help individuals gain insight and validation into their own experience on the spectrum. Additionally, our therapists are trained to assist patients with autism in developing social skills, emotional regulation, sensory sensitivity, and executive functioning skills. Based on developmental age, the treatment also includes skill building for activities of daily living, social interactions (i.e., dating), and preparing for employment. For younger patients, this involves parent education and skills training.
Parents play a crucial role in advocating for their school-aged children. They may be eligible for an Individualized Education Plan (IEP), offering additional school-based treatments, including occupational, speech, and physical therapies and social skills groups. For college-aged patients, many programs support neurodivergent students, including specific ASD dormitories and other support services offered by local disability centers.
Several community-based resources and recreational support include social skills groups, group therapy, and camp programs for those on the spectrum. Many individuals with autism may benefit from holistic treatments such as equine, music, or aquatic therapy. Michigan has several providers specializing in job training, independent living, etc. Our therapists can help provide resources to navigate these opportunities. Individuals may also be eligible for home-and-community-based services through Michigan’s Waiver Program and Community Mental Health. You can read more about this here: https://www.michigan.gov/mdhhs...
Medical nutrition therapy is also an essential adjunct in the management of ASD. Individuals with ASD often lack vitamins D and C, calcium, folate, magnesium, phosphorus, zinc, and iron. They also tend to have lower macronutrient intakes (energy, carbohydrates, protein, and fiber) due to selective/limited eating preferences, including sensory challenges.
Supplements for ASD therapy include vitamin B6, vitamin C, vitamin D, vitamin B12, fatty acids (omega-3 fatty acids and cod liver oil), melatonin, folic acid, l-carnitine, iron, magnesium, zinc, and copper. Our registered dietitians can develop a personalized nutrition plan to help manage ASD through nutrition rehabilitation.
Share Link: What is the treatment for ASD and what type of support is available?
How effective is treatment for ASD at RCBM?
Treatments and services for individuals with Autism can improve a person’s symptoms and ability to function. Early intervention focused on social skills education.
From a nutrition intervention standpoint, it is important to implement large prospective controlled trials to investigate serum levels of folic acid in individuals with ASD. Studies have found that vitamin B6 and magnesium addiction to a person’s diet reduces anxiety and aggression, improves eye contact, increases intelligence quotient (IQ), and improves social interaction. In a recent double-blind, randomized controlled trial involving oral vitamin D supplementation (300 IU vitamin D3/kg/day), it was found that children with ASD significantly reduced core ASD symptoms as a result of supplementation compared to the control group.
Share Link: How effective is treatment for ASD at RCBM?
How do I get started with ASD treatment at RCBM?
If you are interested in treatment at RCBM, you can initiate the admission process by completing a new patient registration form. Once you submit the form, we will match you with one of our qualified clinicians who specializes in treating ASD. Please note that individuals must be residents of Michigan. We are committed to helping you, or your loved one live a quality life and look forward to working with you.
Share Link: How do I get started with ASD treatment at RCBM?
Yvonne Stumpf, MSN, RN, CS, NP, explains Autism Spectrum Disorder (ASD) and our services at RCBM.
Watch: Expert Insights on Autism Spectrum Disorder

Autism Spectrum Disorder
Yvonne Stumpf, MSN, RN, CS, NP explains Autism Spectrum Disorder (ASD) and our services at RCBM.
ASD and Testing Accommodations
Ashley Ceresnie, PhD, LP discusses how full psychological evaluations help school age children through adults understand IQ, academic achievement, along with emotional and social functioning. RCBM provides an in depth assessment for learning differences, ASD and testing accommodations. A detailed report follows testing along with a feedback session to review results and tailor a treatment plan to meet individual needs.Meet the Providers Who Offer Care for Autism Spectrum Disorder

Alexandra Siegel, MA, LLP
Read More

Allison McKee, LMSW
Read More

Ashley Ceresnie, PhD, LP
Read More

Jillian Fortain, PhD, LP, NCSP
Read More

Katherine Huyghe, LMSW (formerly Tessmar)
Read More

Rachel Kwiatkoski, LMSW
Read More
Taylor Drozd, LMSW
Read More

Yvonne Stumpf, MSN, RN, CS, NP
Read More
CareSynch Program
As part of our ongoing commitment to your safety and wellness, we require an annual in-person visit at our office for any patients prescribed controlled substances or GLP-1 medications, along with patients whose primary insurance is Medicare.
The CareSynch program is implemented to ensure the highest standard of care and in response to current and potential regulatory changes. Additionally, please be aware that some pharmacies now require in-person visits before covering specific prescriptions, making these visits even more important.
Please note that this visit will not be with your primary prescriber but with a dedicated CareSynch clinician unless you currently see your provider in the office. If your prescriber is regularly in the office, you can see them for your in-person visit, even if you have routinely been seeing them on Zoom. Please note that a CareSynch appointment will not serve as a medication review.
Our team will contact you to schedule you for this appointment. Visits will be scheduled Monday through Friday from 9 a.m. to 5 p.m. and will be booked for 20 minutes. We understand that some patients will need to travel a distance. We will work with you to find a date that fits your schedule.
You will be seen at our physical location:
https://www.rcbm.net/behavioral-medicine/contact/
Thank you for your cooperation, and we look forward to seeing you at our office.
FAQs
Why do I have to come in for an in-person visit?
Although regulations are evolving, many pharmacies and payors now require at least one in-person visit annually to continue covering medications. This ensures compliance with guidelines and comprehensive care.
Share Link: Why do I have to come in for an in-person visit?
What can I expect from my CareSynch visit?
During your visit, you will meet with one of our dedicated CareSynch clinicians, who will:
- Take your vitals.
- Perform a physical and neurological examination.
- Provide you with any necessary lab requisitions**.
*Other components of your visit will depend on your specific medication regimen, ensuring that all aspects of your care are addressed.**
Share Link: What can I expect from my CareSynch visit?
How do I schedule my CareSynch visit?
Our office will contact you via text with a link to self-schedule your appointment at your convenience.
If you have any further questions, feel free to contact our office.
Share Link: How do I schedule my CareSynch visit?
How long can I expect to be in the office for my visit?
The visit will take approximately 20-30 minutes, ensuring your time is respected while addressing your needs.
Share Link: How long can I expect to be in the office for my visit?
If I already see my provider in the office, do I still need to schedule a CareSynch visit?
- If you see your therapist in the office but not your prescriber, you will need to schedule a CareSynch visit.
- If you already see your prescriber in person at least once per year, there’s no need for an additional visit.
Share Link: If I already see my provider in the office, do I still need to schedule a CareSynch visit?
**Note: If you have had lab work done at your healthcare provider's office within the last year, you may provide your lab work results in lieu of the lab work that is ordered at your CareSynch visit. Results must include:
- Comprehensive Medabolic Panel (CMP)
- Complete Blood Count (CBC) with differential
- Lipid panel
- Vitamin D, 25-Hydroxy
- Vitamin B12/Folate, serum panel
- Thyroid Stimulating Hormone (TSH) with reflex
Meet the Providers Who Offer Care for CareSynch Program
Joel L. Young, MD, Medical Director and Founder
Read More

Ashley Shaow, PA-C
Read More

Brady Brower, PA-C
Read More

James Bolday, MA, Front Office Associate and Medical Assistant
Read More

Rachel Ford, PA-C
Read More
CBT-I

Over 50% of adults report difficulty sleeping, half of which suffer with chronic sleep difficulty. We now know that medications are not the only solution to insomnia and that it is possible to successfully treat insomnia using cognitive-behavioral therapy (CBT). CBT has been endorsed by the National Institutes of Health as an effective method for treating insomnia. Research on CBT shows the following:
- 75% of insomnia patients experience significantly improved sleep
- The majority become normal sleepers
- 85- 90% reduce or eliminate sleeping pills
CBT achieves these results because it is based on the idea that insomnia is treated effectively by addressing the underlying causes of insomnia-related thoughts and behaviors, which are learned and can be unlearned.
CBT-I COMPONENTS
Techniques taught in CBT-I include:
- Changing sleep thoughts and behaviors
- Lifestyle habits that improve sleep
- Relaxation techniques
WHO WOULD BENEFIT
- Individuals with problems falling asleep, waking during the night, or waking too early
- Individuals who wish to avoid, reduce, or eliminate sleep medications
VISITS
CBT for insomnia includes:
- Five individual treatment sessions over a six-week period (Sessions 1-3 once per week, skip a week, session 4, skip a week, session 5)
INSURANCE COVERAGE
CBT-I is billed as a psychotherapy visit
PARTICIPANT REPSONSIBILITIES
- Weekly reading in book that participant purchases called “Say Goodnight to Insomnia”
- Weekly reading of the session summary handout that accompanies the book
- Daily writing of sleep information in “sleep diary” log
- Daily writing of a negative and positive sleep thought on provided "thought log"
- Practicing guided relaxation using MP3 audio provided via email
- Practicing sleep modification behaviors and other habit changes as guided by the program
.jpg)
Watch: Expert Insights on CBT-I

What is CBT-I?
Julia Rodgers, BSN, LLMSW explains RCBM's CBT-I program - a - 6 week treatment program that focuses on identifying, along with changing thinking, feeling and behaving that contributes to sleep challenges. CBT-I is the gold standard of care for insomnia.
CBT-I and Chronic Insomnia
Julia Rodgers, BSN, LMSW heads the cognitive behavioral therapy program for insomnia. She presents approaches used at RCBM including targeting unhelpful sleep thoughts and behaviors, and addressing the root cause of insomnia through CBT-I by exploring fears. while shifting thinking and behavior.Child and Family Services
Our goal is to help your child lead the most normal and successful life possible. Through therapeutic work with the child, the family, and the school, we can help you navigate your child's diagnosis and create peace of mind for you and your child, along with harmony within your household. At RCBM, we believe that many diagnoses relate to the family. Many diagnoses can begin in childhood. Together, with an appropriate clinician and treatment plan, the child and family can experience successful treatment. For the child, we provide psychotherapy, medication management, and counseling for school-related issues (learning, discipline, academia, anxiety, etc). For the parents, we provide individual, couples, and family therapy for respective issues related to the family. Whether you are dealing with a life adjustment or an issue such as the loss of a loved one or a terminal illness, RCBM is here to offer our full support to you, your child, and your family.
Meet the Providers Who Offer Care for Child and Family Services
Allison McKee, LMSW
Read More

Ashley Crowder, LPC
Read More
Ashley Ceresnie, PhD, LP
Read More

Bryn Thompson, PA-C
Read More

Holly Watt, LMSW
Read More
Katherine Huyghe, LMSW (formerly Tessmar)
Read More

Libby Quail, MA, LPC
Read More

Lindsey Kennard, MA, LPC (formerly Mandell)
Read More

Lisa Michaux, MSN, PMHCNS-BC
Read More

Mckenzie Lopez, LMSW
Read More
Taylor Drozd, LMSW
Read More
Yvonne Stumpf, MSN, RN, CS, NP
Read More
Cognitive Behavioral Therapy

The Rochester Center for Behavioral Medicine uses Cognitive Behavioral Therapy (CBT) for the treatment of anxiety and depressive disorders. This therapy combines behavioral exposure therapy and cognitive restructuring to help the patient confront avoidance, correct negative automatic thoughts, and return to optimal functioning.
CBT is particularly effective for, but not limited to, the Anxiety Disorder spectrum, such as Panic Disorder, Post Traumatic Stress Disorder, Obsessive Compulsive Disorder, Social Anxiety Disorder, and Specific Phobias. The hallmark of CBT is the patient’s role in learning and practicing skills outside the session to maximize the therapeutic benefit of this therapy. In mood disorders, the patient will learn coping skills to master tasks often thought too arduous for the depressed patient. The use of CBT with or without medication management is addressed, and the ultimate decision is made between the patient and the RCBM Professional.
FAQs
What is Cognitive Behavioral Therapy (CBT)
Cognitive Behavioral Therapy (CBT) is a structured, goal-oriented psychotherapy that helps people identify and change negative thought patterns and behaviors. By changing thoughts, one can change how they feel, such as reducing depression, anxiety, and anger.
It is often used to treat a variety of mental health conditions. CBT focuses on the connection between thoughts, emotions, and behaviors. By identifying unhelpful thoughts and replacing them with more constructive ones, individuals can improve how they feel and respond to challenges. CBT is typically a short-term therapy, lasting anywhere from 6 to 20 sessions, depending on the individual and the condition being treated. Extensive research shows that CBT is highly effective for many mental health issues. Its structured approach and focus on skill-building often lead to lasting improvements.
CBT is focused on the present and problem-solving-oriented. CBT will assist you in learning skills to identify distorted thinking/distressing thoughts, modify beliefs, relate to others in different ways, replace thoughts, and change behaviors. In addition, CBT will help you connect thoughts, feelings, and behaviors, change your mood/feelings by thinking more realistically, and decrease negative behaviors.
Share Link: What is Cognitive Behavioral Therapy (CBT)
What conditions can CBT help with?
CBT is one of the most studied treatment interventions, effective with a wide range of disorders. It is commonly used for:
- Anxiety disorders (e.g., generalized anxiety, social anxiety)
- Depression
- Post-traumatic stress disorder (PTSD)
- Obsessive-compulsive disorder (OCD)
- Eating disorders
- Phobias
- Insomnia
- Substance abuse
Share Link: What conditions can CBT help with?
What happens in a CBT session?
In a CBT session, you will:
- Discuss current issues and symptoms.
- Identify negative thought patterns.
- Learn strategies to change these patterns and behaviors.
- Practice new skills in and outside of sessions.
Homework is a key component of CBT. You might track your thoughts, practice techniques, or test new behaviors in real-life situations.
Share Link: What happens in a CBT session?
How do I get started with CBT at RCBM?
If you are a current patient at RCBM, please contact our office at (248) 608-8800. If it has been more than three years since you have had diagnostic screening, we will need to re-administer before treatment. If you are new to RCBM, please complete our new patient registration form to start the admission process.
Individuals must reside in Michigan and be willing to come to the office if needed.
We look forward to helping you feel better!
Share Link: How do I get started with CBT at RCBM?
Related Titles from the RCBM Reading and App list:
Feeling Great: The Revolutionary New Treatment for Depression and Anxiety - By David BurnsAlarmy - App to help people wake up
CBT Thought Record Diary
MindShift
Pacifica - Anxiety, Stress, & Depression relief
Comprehensive Psychiatric Evaluation & Second Opinions

Navigating mental health concerns can sometimes lead to complex questions about your diagnosis or treatment plan. At the Rochester Center for Behavioral Medicine, we offer comprehensive psychiatric evaluations to provide clarity and confidence in your mental health journey. If you're uncertain about your current diagnosis or are exploring how to find the right psychiatrist, our team is here to assist.
Our Services:
● Independent Evaluations: Led by our Medical Director, Joel L. Young, MD, our independent psychiatric examinations delve deep into your mental health history and current concerns. This thorough approach ensures that we address all facets of your well-being.
● Second Opinions: Mental health diagnoses can be intricate. Seeking a second opinion can offer new perspectives, especially if you're experiencing persistent symptoms or have reservations about your current treatment plan. Our evaluations are designed to provide comprehensive insights, helping you understand the signs you may need therapy or adjustments in your current approach.
Integrated Support:
Beyond evaluations, RCBM offers a spectrum of services to support your mental health:
● Therapeutic Services: From individual therapy to cognitive behavioral therapy (CBT), our licensed therapists employ evidence-based techniques to address various mental health challenges.
● Specialized Programs: For concerns like dementia, our Dementia and Cognitive Evaluation Program offers targeted assessments and interventions.
Take the Next Step:
Understanding your mental health is a vital aspect of overall well-being. If you're contemplating a comprehensive evaluation or seeking a second opinion, reach out to us at (248) 608-8800. Our team is dedicated to guiding you toward clarity and improved mental health.
Comprehensive Psychological Evaluations and Testing

A comprehensive psychological evaluation is a process that helps individuals from school age through adulthood understand their cognitive abilities (also known as IQ), academic achievement, and emotional and social functioning.
At RCBM, our screening and comprehensive psychological evaluation programs serve distinct but complementary roles in the diagnostic process. Diagnostic screening is always the first step—a targeted assessment to identify symptoms, guide accurate mental health diagnoses, and support a treatment plan.
If diagnostic screening results indicate that additional information is needed to fully understand cognitive abilities (IQ), academic achievement, or social/communication behaviors, or if an individual requests, we recommend a more thorough, comprehensive psychological evaluation. These academic and cognitive evaluations can provide a deeper understanding of how an individual learns and may be especially helpful when considering educational planning, accommodations, or other support services tailored to their unique needs.
Patient Interest Form for Comprehensive Psychological Testing
Please complete the interest form for comprehensive psychological testing, which includes evaluations for specific learning disorders, accommodation testing, guardianship evaluations, and other related services. The evaluation is done in person.
Learn about the various comprehensive psychological evaluations we offer below, along with detailed information about the process.
FAQs
What are specialized psychological evaluations and how do they work?
- Specialized psychological evaluations evaluate for specific concerns, including learning disorders, cognitive decline, and Autism Spectrum Disorder
- Often used to establish a diagnosis for supports, accommodations, and services
- Conducted by RCBM psychologists
- Completed in the clinic
Share Link: What are specialized psychological evaluations and how do they work?
Specific Learning Disorders Evaluation
Specific Learning Disorders are impairments in Reading, Mathematics, and/or Writing (previously known as Dyslexia, Dyscalculia, or Dysgraphia). RCBM works with patients, their families, and schools to support educational planning after evaluations. These evaluations begin with a thorough psycho-social history and review of academic data.
The evaluation includes the following:
- An assessment of intellectual/cognitive abilities (I.Q.), including an evaluation of their verbal reasoning, perceptual reasoning, working memory, and processing speed skills
- A comprehensive evaluation of academic skills, examining reading, writing, and/or math skills
Share Link: Specific Learning Disorders Evaluation
Intellectual Disability Evaluation
Intellectual Disabilities include deficits in both intellectual and adaptive functioning. These evaluations begin with a thorough psycho-social history and review of educational data.
The evaluation includes the following:
- An assessment of intellectual/cognitive abilities (I.Q.), including an evaluation of their verbal reasoning, perceptual reasoning, working memory, and processing speed skills
- A comprehensive assessment of academic skills, examining reading, writing, and/or math skills
- Adaptive Behavior rating scales
Share Link: Intellectual Disability Evaluation
Guardianship Evaluation
Many times, individuals with disabilities require a need for parents or loved ones to request guardianship from the state to support their family members with ongoing assistance, daily living care, and help with financial and medical decision-making. At RCBM, we work with families to understand the legal considerations to evaluate an individual’s abilities, academic skills, social/emotional functioning, and adaptive behavior as part of the guardianship application process. These evaluations begin with a thorough psycho-social history and review of educational data and pertinent medical records.
The evaluation can include the following:
- An assessment of intellectual/cognitive abilities (I.Q.), including an evaluation of their verbal reasoning, perceptual reasoning, working memory, and processing speed skills
- A comprehensive assessment of academic skills, examining reading, writing, and/or math skills
- Adaptive Behavior and/or other behavioral rating scales
Share Link: Guardianship Evaluation
Accommodations/High Stakes Evaluations
RCBM also offers accommodation evaluations for high-stakes exams such as the SAT, ACT, LSAT, MCAT, and GRE. We provide the evaluation required by each testing agency to document symptoms and make appropriate diagnoses (or update previous testing/documentation) for accommodations. These accommodations can include extended time, extra breaks, small group testing, etc.
Share Link: Accommodations/High Stakes Evaluations
Comprehensive Psychological Evaluation Timeline
Following the diagnostic assessment, the comprehensive psychological evaluation has three components. All components are individualized based on the referral.
Intake
- One hour
- Conducted virtually
- It will be discussed if additional tests, record reviews, or interpretations are required based on the referral.
Evaluation
- Approximately four hours
- In-person at our office
Feedback
- Scheduled three to five weeks after completion of the evaluation to review the findings and recommendations
- The time required varies depending on the referral concerns and individual needs
Share Link: Comprehensive Psychological Evaluation Timeline
Cost information
While the intake and feedback sessions are billable to insurance companies, the in-person evaluation component is not billable to any insurance. The cost of the evaluation will be able to be determined once the referral is made or interest form is completed.
Share Link: Cost information
If you have any questions regarding our psychological evaluation program or other academic and cognitive evaluation requests, please contact Ashley Ceresnie, PhD,
Director of Comprehensive Psychological Evaluations at aceresnie@rcbm.net.
Watch: Expert Insights on Comprehensive Psychological Evaluations and Testing

What is a Comprehensive Psychological Evaluation
Ashley Ceresnie, PhD, discusses RCBM's Comprehensive Psychological Evaluation and Testing Services for learning differences, ASD, and testing accommodations.
Full Psychological Evaluation
Ashley Ceresnie, PhD oversees RCBM's full psychological evaluations. She discusses when a full psychological evaluation is indicated based on what families notice in their child such as academic challenges, including keeping up, focus, organization and planning, or social and emotional concerns that affect overall wellbeing. A full evaluation can be indicated for school age to adults and measures cognitive abilities, academic achievements, emotional and social functioning, how an individual thinks, learns, communicates and manage everyday demands to guide individual treatment.Meet the Providers Who Offer Care for Comprehensive Psychological Evaluations and Testing
Ashley Ceresnie, PhD, LP
Read More

Ines Hadziegric, MA
Read More
Couples Counseling

Couples therapy at RCBM is a collaborative process designed to help partners build stronger, healthier relationships. Whether you're facing specific challenges or simply looking to enhance your connection, RCBM’s couples therapists offer a supportive environment for partners to learn how to engage with each other more effectively. You and your partner will learn to identify unhelpful communication patterns, recognize how you trigger one another, and develop strategies to manage negative emotions. Committing to couples therapy is a courageous step toward healing, growth, and creating the kind of relationship you both desire. Whether you're experiencing high conflict, feeling emotionally distant, or simply want to fine-tune your connection, couples therapy can be a powerful and effective resource for lasting relationship health.
Who is couples therapy for?
Couples therapy can be suitable for any relationship. It’s most common for married partners to seek couples therapy, but it can help improve any relationship. Relationships between parents and children, siblings, co-workers, friends, and relatives can all be improved through couples therapy.
What can we expect in couples counseling?
For couples counseling to be effective, it’s essential that each person be willing to look at their contribution to the dysfunction between them. Although it is common for each member of the dyad to build a strong case for why the other person should change, for any relationship to improve, it’s imperative that each person focus on what they can do differently to build a more respectful and satisfying relationship.
How can we get the most out of couples counseling?
It’s crucial for the success of therapy that each person consider what they hope to accomplish in each session and actively choose a focus for the day. It is helpful when each person reflects on the outcome they desire from each session. To help you better understand our approach to working with couples, we have created this document to provide some insight into what you can expect during our work together. In addition, here is a recommended reading list for couples.
FAQs
What are some typical areas to focus on in a couple’s therapy session?
- What would you like to be experiencing that you aren’t experiencing now?
- What are you longing for in this relationship?
- What is most distressing about your interaction?
- In what ways would you like your relationship to be different?
Share Link: What are some typical areas to focus on in a couple’s therapy session?
What is the number one presenting problem in couples counseling?
Communication is the number one presenting problem in couples counseling, followed closely by lack of connection and feeling unseen.
Share Link: What is the number one presenting problem in couples counseling?
How will couples therapy assist us in communicating more effectively?
Throughout couples therapy, you will learn how to incorporate the following strategies when engaging in difficult conversations
- Active listening
- Using “I” statements
- Paying attention to nonverbal cues
- Remaining curious
- Displaying empathy
- Staying open
- Willingness to compromise
- Recognize triggers
- Emotional regulation
- Uncovering vulnerability
- Taking time-outs
Share Link: How will couples therapy assist us in communicating more effectively?
What can we expect during the first few sessions of couples therapy?
The first few sessions will involve gathering background information, highlighting relationship concerns, and expectations for future treatment. You and your partner will meet together for session one. Then, each of you will meet individually. You will come back together for session four at which time goals will be discussed and a treatment plan formalized.
Share Link: What can we expect during the first few sessions of couples therapy?
Why is it recommended that each of us be in our own individual therapy while attending couples therapy?
Over the course of couples counseling, partners will discover unique sensitivities, or triggers, that, when activated, impede healthy communication. Once these triggers are illuminated, partners can explore them more deeply with their individual therapist. As a result, partners gain a heightened understanding of their internal world, learn self-regulation strategies, and come to understand when and why their triggers get activated. These skills help support and expedite the work being done in couples therapy.
Share Link: Why is it recommended that each of us be in our own individual therapy while attending couples therapy?
How do we get started in couples counseling?
If you are a current patient at RCBM, don't hesitate to contact our office at (248) 608-8800. If you are new to RCBM, please complete the new patient registration form. Once you submit the form, we will match you with one of our qualified therapists.
Please note that individuals must be residents of Michigan. We are committed to helping you and look forward to working with you.
Share Link: How do we get started in couples counseling?
Marni Stone, LMSW, is a graduate of the Couples Institute. In this video, she discusses how she can help couples and families with communication skills, coping techniques, patterns of interaction, and other important areas of stress.
Meet the Providers Who Offer Care for Couples Counseling

Marni Stone, LMSW
Read More

Amy Karwowski, LMSW
Read More

Angela Eddy, MA, LPC, NCC
Read More
Ashley Crowder, LPC
Read More

Aundreah Walenski, LMSW
Read More
David Price, MA, LPC, CAADC
Read More

Jennifer Lindsey, LMSW
Read More

Kaca Popovic, MA, LPC
Read More

Karolina Redziniak, MA, LLP
Read More
Katherine Huyghe, LMSW (formerly Tessmar)
Read More

Kelly Dahl, LMSW
Read More
Lisa Robinson, MA, LPC, CAADC
Read More
Matthew Barsenas, LMSW, JD
Read More
Dementia / Cognitive Evaluations

For some patients, it is essential to assess cognitive functions, including memory, recall, alertness, and overall cognitive aptitude. This is formally done by neuropsychological and psychological testing. This type of testing can be ordered following a medical illness, such as stroke or other brain-based diseases, such as Parkinson's Disease or Multiple Sclerosis. Psychological testing is also ordered to evaluate dementia. Dementia is the diminution in cognition and memory. It is associated with the aging process. The most common type of dementia is Alzheimer's Type. These are important diagnoses to make early on. Some dementias are reversible if caught early. For other types, such as Alzheimer’s and vascular dementias, newer cognitive enhancing medications are available that can improve functioning and prolong quality of life.
What is the difference between cognitive decline and dementia?
Cognitive decline refers to a gradual decline in cognitive function, affecting memory, thinking, learning, and communication. It can be a normal part of aging or can be influenced by various health factors and lifestyle choices. Not everyone who experiences cognitive decline will develop a more serious condition.
Dementia, on the other hand, is a specific medical diagnosis characterized by a significant decline in cognitive function that interferes with daily life and activities. It encompasses a range of symptoms, including memory loss, difficulty with communication, impaired reasoning, and changes in mood or behavior. Dementia is caused by various underlying conditions, with Alzheimer's disease being the most common.
While cognitive decline can be a general term for a decrease in mental abilities, dementia is a diagnosable condition that involves more severe cognitive impairment affecting daily functioning.
What Are Dementia & Cognitive Evaluations?
- Our evaluations help identify the cause of memory loss, confusion, and other cognitive changes.
- We provide clear diagnosis and guidance to support treatment planning and care.
Who Can Benefit?
- Adults experiencing memory problems, confusion, or difficulty with daily tasks
- Family members concerned about a loved one’s cognitive health
- Individuals seeking a second opinion or formal diagnosis for dementia or related conditions
What to Expect
- Initial consultation with a psychiatric provider
- In-depth cognitive testing using standardized tools
- Feedback session to review results and next steps
Why Choose RCBM?
- 30+ years of experience in behavioral and cognitive health
- Integrated team of psychiatrists, neuropsychologists, and licensed clinicians
- Collaborative care that includes the patient, family, and referring providers
Watch: Expert Insights on Dementia / Cognitive Evaluations
Virtual Therapy | with Joel L. Young, M.D., Rochester Center for Behavioral Medicine
Dr. Joel Young, Medical Director and founder of the Rochester Center for Behavioral Medicine discusses Virtual Therapy during the Coronavirus pandemic, and beyond. We explore the use of Cutting-edge technology as a win win for both patients and therapists. Will this become the new normal?Diagnostic Screening

What conditions are evaluated?
Our Diagnostic Screening process quantifies the extent of a wide variety of mental health conditions. For adults, we screen for over 60 mental health conditions, including:
- Anxiety Disorders
- Depressive Disorders
- ADHD and its various subtypes
- Trauma-related disorders
- Chronic Fatigue and Sleep Disorders
- Substance use disorders
- Eating disorders
- Personality Disorders
For children and adolescents, neurocognitive functioning can be assessed remotely as a part of diagnostic screening. Other aspects of diagnostic screening can include evaluating and offering guidance regarding career planning.
ADHD and Comorbidities
Diagnostic screening is beneficial for the assessment of comorbidities. Comorbidities occur in 25% to 45% of individuals with ADHD. Common ADHD comorbidities include:
- Anxiety Disorders
- Depression
- Learning disorders
Input from teachers and family is included in your final report, which will be generated upon completion of diagnostic screening.
What happens after screening is completed?
Your RCBM clinician will meet with you to review your results and develop a comprehensive treatment plan, which may include:
- Medication management
- Psychotherapy
- Medical nutrition therapy and/or coaching
Where can I find more information?
The following contains frequently asked questions about the process for our diagnostic screening services. If you have already been referred for Diagnostic Screening and have additional questions after carefully reviewing the FAQs below, don't hesitate to contact your Screening Team Psychometrician directly via their email address.
FAQs
What is diagnostic screening and how does it work?
- Diagnostic screening assesses for symptoms of up to 60 psychiatric conditions.
- Results help clarify your diagnoses and informthe treatment plan
- Our psychometric team administers testing under a licensed psychologist's supervision
- Assessments are primarily completed independently online but may include a proctored component (if needed).
Share Link: What is diagnostic screening and how does it work?
What does the diagnostic screening process entail?
I would like to complete Diagnostic Screening. What are the next steps?
To complete Diagnostic Screening, you must have an appointment and be referred for Diagnostic Screening by one of RCBM’s licensed clinicians. Currently, we do not offer our screenings as a stand-alone, outside service to non-patients.
New Patients: If you are not already a patient at RCBM, please visit https://www.rcbm.net/behavioral-medicine/first-visit/ and complete the “New Patient Pre-Registration Form.” After you submit that form, our patient coordinator will contact you to discuss the next steps
Current Patients: If you are already a current patient at RCBM – meaning you have been seen by one of our providers in the past six months – please talk to your provider about completing diagnostic screening.
Once a clinician submits a referral form, a contract will be automatically sent to you. When you complete the contract, a screening team member will assign you to a psychometrician, and screening materials will be sent within 5 business days.
What does the Diagnostic Screening process entail?
For all age groups, assessments are currently completed online from the comfort of the patient’s home. RCBM is NOT conducting in-office screening at this time.
Adults (18+)
Self-Report Data: Adult patients will generally complete screening in two parts. Part 1 contains 2-5 links, and Part 2 includes one direct assessment link. Additional assessments may be assigned if requested by the clinician. You will receive an email from your assigned psychometrician with the links to the assessments. Once all assessments (links) are completed, your assigned psychometrician will review the results and may send additional assessments for further evaluation. An email will be sent if this is the case. If no additional assessments are needed, the psychometrician will require 2-3 business days to process your data, and results will be requested by the next business day.
Observer Data: Data is also collected from another person in the Adult patient’s life who knows them well. For screening purposes, this person is called an “Observer” and is usually one’s partner, roommate, parent, or close friend. The “Observer” completes two short assessments based on their observations of you, the patient.
Teens (ages 13-17)
Self-Report Data: Teens typically complete the screening in two parts. Part 1 contains 2-3 links, and Part 2 includes 1 direct assessment link. Additional assessments may be assigned if requested by the clinician.
Parent Data: We ask each parent to complete several assessments about their teen’s behavior and functioning. Each parent will receive their own set of screening materials in one part, containing 2-3 links. A singular parent will receive Part 2, which includes one direct assessment link. Each parent should complete their set of assessments individually.
Teacher Data: Your teen’s teacher will be asked to complete 2-3 rating scales about your child’s behavior and functioning in their current academic setting. Please see the “Teacher Collection” FAQs section for RCBM’s teacher data collection requirements.
Children (ages 8-12)
Self-Report Data: Children typically complete the screening in a single email containing 1-3 Parts and 4-7 links.
Parent Data: We ask each parent to complete several assessments about their child’s behavior and functioning. Each parent will receive their own set of screening materials in two parts: Part 1 contains one link, and Part 2 includes 2-3 links. Each parent should complete their set of assessments individually.
Teacher Data: Your child’s teacher will be asked to complete 2-3 rating scales about your child’s behavior and functioning in their current academic setting. Please see the “Teacher Collection” FAQs section for RCBM’s teacher data collection requirements.
Younger Children (ages 4-7)
Self-Report Data: No Self-Report assessments are completed by children in this age group.
Parent Data: We ask each parent to complete several assessments about their child’s behavior and functioning. Each parent will receive their own set of screening materials in two parts: Part 1 contains one link, and Part 2 includes 2-3 links. Each parent should complete their set of assessments individually.
Teacher Data: Your child’s teacher will be asked to complete 2-3 rating scales about your child’s behavior and functioning in their current academic setting. Please see the “Teacher Data Collection” FAQs section for RCBM’s teacher data collection requirements.
Share Link: What does the diagnostic screening process entail?
Screening timeline
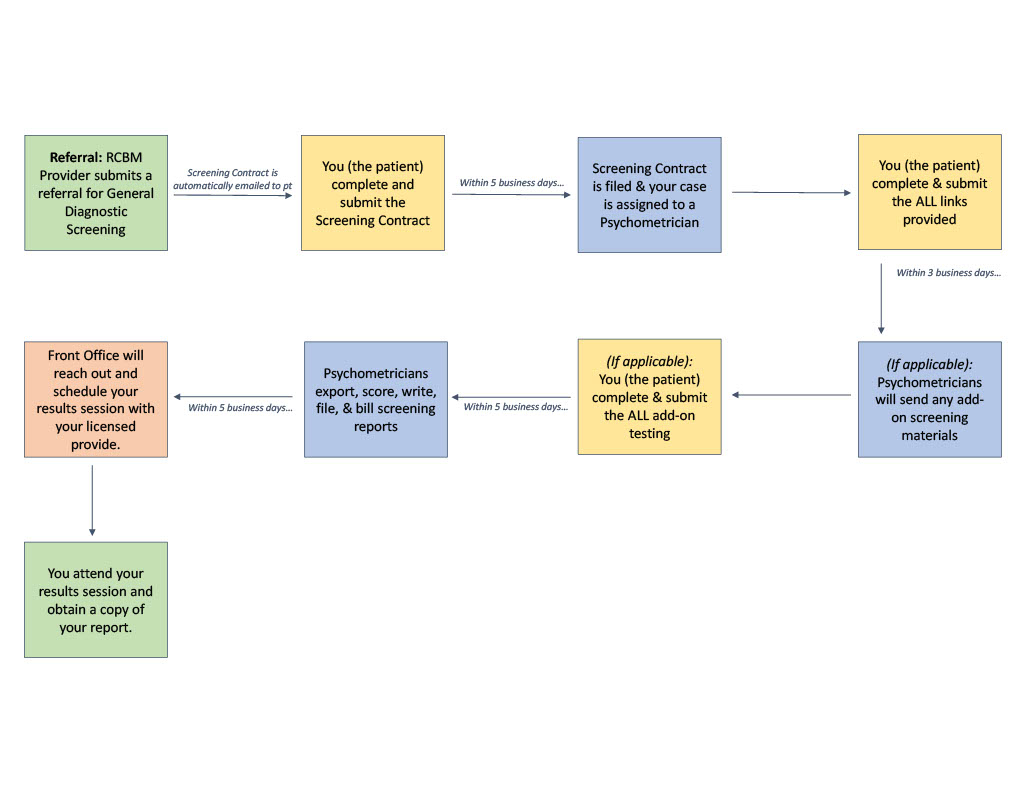
I do not have a computer, but I do have an iPad/tablet or iPhone. Can I still complete the screening assessments?
All assessment links can be completed on an iPad/tablet, except for CNS Vital Signs (i.e., Part 3 for children and adolescents ages 8-17, or Part 5 in some adult screenings ages 18+). To run correctly, the CNS Vital Signs assessment must be completed on a computer. Please do not use a cell phone to complete the diagnostic screening assessments.
Share Link: I do not have a computer, but I do have an iPad/tablet or iPhone. Can I still complete the screening assessments?
Billing and payment
What does screening cost, and does my insurance cover it?
Full payment is due upon completion of screening. The cost you are responsible for will be reflected on your monthly billing statement, or you can view your account balance by logging in to the patient portal shortly after screening is completed. We encourage patients to reach out to our billing staff, Alana Gillespie (agillespie@rcbm.net) and James Fields (jfields@rcbm.net), to arrange a payment plan, if desired or necessary.
Insurance coverage of diagnostic screening (procedure codes 96138 and 96139) varies by plan. If it is covered, please note that you will be responsible for your deductible and one co-pay/coinsurance per screening unit (half hour). If it is not covered, you will be responsible for payment in accordance with RCBM’s Private Pay fee schedule.
Ultimate payment responsibility rests with the patient.
Is Diagnostic Screening billable to my insurance?
Diagnostic Screening at RCBM is a billable service to certain BCBS-PPO, BCBS-Federal, Aetna, Cigna, and Medicare Plus Blue plans only*.
· *Please be aware of mental health care outs: Some insurance policies have a “carve out” where mental health benefits are provided through a contract with a separate provider or insurance company. For example, some BCBS medical insurance plans have a carve-out that requires all mental health claims to be submitted and processed by Carelon Behavioral Health. Our screening is NOT billable to Carelon Behavioral Health, and therefore, patients with this carve-out plan will be responsible for the Private Pay fee for Diagnostic Screening.
· *BCBS PPO through Ascension typically does NOT cover the diagnostic screening provided by RCBM. The Billing Department will bill Ascension BSBS for the diagnostic screening. Please note that if the claim is denied, you will be responsible for the out-of-pocket screening costs.
· *Note that ONLY Medicare through BCBS – the Medicare Plus Blue plan – is billable for screening. Screening cannot be billed to any other Medicare plans.
This information is NOT a guarantee of benefits or payment. If your insurance company is billed and you have not met your deductible, you can expect to pay between $150.00 and $400.00, depending on the services performed and the patient’s age.
Private Pay Rates: If your insurance carrier is not listed above, RCBM is *not able to bill* your diagnostic screening to your insurance, and you will be responsible for the Comprehensive Diagnostic Screening Private Pay rate of $350.00 for individuals ages 8+; $250.00 for individuals ages 4-7.
The contract states Diagnostic Screening is not billable to my insurance, but I called my insurance company, and they said that it is billable. So is it billable?
RCBM’s Diagnostic Screenings are conducted by trained psychometricians under the supervision of Joel L. Young, MD, Medical Director. RCBM’s psychometricians are responsible for scoring the data and compiling it into the patient’s diagnostic screening report. Some insurance companies only cover screening or assessment services completed by a licensed mental health clinician (e.g., LP, LLP, LMSW, LPC, etc.) and do not cover assessments completed by psychometricians.
If our website states that we are unable to bill your insurance, your insurance does not cover diagnostic screening completed by trained and supervised psychometricians.
If the 96138 and 96139 codes are a covered benefit on your insurance plan, but are not billable to your insurance by RCBM (because we are not “in-network” for screening/evaluation services specifically), you have the option of finding an in-network provider to perform the screening. *If you proceed with the Screening at RCBM, you are responsible for out-of-pocket payment of this service.*
*Note. All diagnostic interpretations are made by one of RCBM’s licensed clinicians.
Diagnostic Screening was once billable to my insurance but according to the contract, now it is not billable. Is this correct?
Diagnostic Screening billing codes and contracts may change. If our contract indicates that this code is not billable to your insurance, this is the most current information we have.
What if I cannot pay for screening and do not want to proceed due to the cost of Diagnostic Screening?
(agillespie@rcbm.net) and James Fields (jfields@rcbm.net) to discuss payment plan options.
If you have contacted our billing department and do not want to proceed with screening, please contact your clinician regarding how this may impact your care and treatment planning. Please notify your assigned psychometrician via email so they may update your chart.
Share Link: Billing and payment
Observer forms for adults
What are the Observer Forms? If I do not have anyone to complete the Observer Forms, can I still complete screening?
- If you are an Adult and participating in diagnostic screening at RCBM, you will be asked to provide the name and email address for an “Observer” on the Screening Contract form.
- Observer Data is collected from one person in an Adult patient’s life who knows them well. This person is referred to as an “Observer” and is usually a partner, roommate, parent, or close friend.
- The “Observer” completed one short assessment about the Adult patient’s recent behavior and functioning.
- It is highly recommended that all Adults completing the Screening provide the name and email address of an “Observer.” This allows your clinician to look for patterns across reports (you and the observer) in the screening data and can aid in obtaining an accurate diagnosis.
- Please let your psychometrician know if you did not provide an Observer’s contact information on the Screening contract, but would like to do so now.
Share Link: Observer forms for adults
Teacher data collection for children and teens
Why is teacher data so important for Diagnostic Screening?
We strongly encourage you to provide the contact information for one teacher on the screening contract. Your child spends several hours every day at school, surrounded by peers and responding to a variety of task demands and unique situations not often encountered at home or in the community. Teachers provide valuable observations of your child’s daily behavior and functioning at school.
At RCBM, we highly value teacher input for many reasons. Most notably, the teacher’s school-based data plays an essential role in ensuring that your child is accurately diagnosed and that appropriate treatments are recommended. In fact, the diagnostic criteria for some conditions require symptoms to be present in multiple settings, such as both home and school.
*Note: For some conditions, RCBM providers may require that teacher data be obtained as part of the screening process for some conditions/cases. The results may be delayed if not completed in a timely manner, and/or some treatment options may be limited without teacher data.
Where do I provide the contact information for my child’s teacher?
On the Screening Contract, you will be asked to provide the name and email address of ONE teacher who knows your child well and ideally teaches a core/academic subject, such as math, language arts, or science.
By providing the teacher’s name and contact information on the Screening Contract, you consent to our contacting them via email and asking them to complete a couple of rating scales about your child.
Who is responsible for making sure my child’s teacher completes their screening materials?
We sent multiple reminders via email to your child’s teacher, prompting them to complete the rating scales. However, ultimately, it is your responsibility to inform your child’s teacher that:
1) They will be receiving these rating scales via email from RCBM
2) They will have about 2 weeks to complete the rating scales online.
Please notify your child’s teacher as soon as you complete the screening contract.
My child is in middle school or high school and has many teachers. Do all of their teachers need to complete a separate Teacher Report form?
No. Please choose only ONE teacher who knows your child well and ideally teaches a core/academic subject (i.e., math, language arts, science) to complete the assessments.
You will be asked to provide this information on the Screening Contract form so we can email the teacher directly. Please let your psychometrician know if you did not provide the name and email address of one of your child’s teachers, but would like us to do so now.
It is highly recommended that we obtain Teacher data for your child. This allows your clinician to look for patterns across reporters (your child, you, the child’s other parent, and a teacher) and across settings (home, school, community) in the screening data and aids in obtaining an accurate diagnosis.
Share Link: Teacher data collection for children and teens
Screening contract and assessment materials
I did not receive the Screening Contract, even though my clinician said I would receive it shortly after my appointment. When can I expect this email to arrive?
- Screening contracts are sent to patients immediately upon completion of a clinician's referral form.
- If you have not received it, please search your email for ”RCBM Screening Contract”.
*Make sure to check your spam/junk folder too!
- If you cannot find the Screening Contract, please get in touch with COMPASS at our General Diagnostic Screening department at screeningteam@rcbm.net or TEXT (248) 609-4483 with your name (or your patient's name, if applicable). You may also contact your clinician at their email address to notify us that you have not received the Screening Contract yet. We will send/resend it to you on the following business day.
I submitted the Screening Contract. When will I receive my Assessments?
- You can expect to receive your diagnostic screening materials within 5 business days of receiving your signed Screening Contract form. The email will have RCBM Diagnostic Assessments in the subject line.
- If it has been more than 5 business days, please search your email for “RCBM Diagnostic Assessments.”
*Make sure to check your spam/junk folder too!
If you cannot find them, please get in touch with COMPASS at our General Diagnostic Screening department at screeningteam@rcbm.net, or with your clinician at their email address, to let us know you have not received the diagnostic screening materials yet. We will send/resend it to you on the following business day.
The Assessment link(s) I was sent are not working. What should I do?
- First, please ensure you complete the assessments in Google Chrome, as they work best in this browser. Check that the web browser is fully expanded to view all the screen contents.
- If the assessment continues to report errors, please clear your browser history and cookies, then try the links again.
- If the problem persists, please contact your psychometrician at their email address, and they will troubleshoot the issue promptly.
Scheduling a Results session and Obtaining the Screening Report.
How soon after I complete screening will I be contacted to schedule my Results appointment?
- After you complete all of the assessments, you will receive a phone call from the RCBM front office to schedule your results appointment.
- You will receive this phone call within 5 business days of submitting your final assessment (excluding holidays).
- If you believe you have completed all of the assessment links and have not received a call to schedule your results appointment after 5 business days, please
- 1) Review the original email sent to you by your Psychometrician and double-check that you have completed all the assessment links, and then
- 2) Contact your Psychometrician via email to confirm all assessments have been completed.
Will I receive a copy of my Diagnostic Screening Report?
- After your results session with your RCBM clinician, you will receive a copy of your report via email. If you do not receive a copy after your session, please contact the Front Office at (248) 608-8800.
Share Link: Screening contract and assessment materials
Scheduling a results session and obtaining the screening report
How soon after I complete the screening will I be contacted to schedule my Results appointment?
- After you complete all of the assessments, you will receive a phone call from the RCBM front office to schedule your results appointment.
- You will receive this phone call within 5 business days from the date you submitted your final assessments (excluding holidays)
- If you believe you have completed all of the assessment links and have not received a call to schedule your results appointment after 5 business days, please
- 1) Review the original email sent to you by your Psychometrician and double-check that you have completed all the assessment links, and then
- 2) Contact your Psychometrician via email to confirm all assessments have been completed.
Will I receive a copy of my Diagnostic Screening Report?
- After your results session with your RCBM clinician, you will receive a copy of your report via email. If you do not receive a copy after your session, please email your psychometrician.
Share Link: Scheduling a results session and obtaining the screening report
Meet the Providers Who Offer Care for Diagnostic Screening

Ava Doerr, BS
Read More

Alyssa Cooley, MA. Screening Team Lead
Read More

Haley Mozen, BA
Read More
Jillian Fortain, PhD, LP, NCSP
Read More

Lauren Ahn, BSW
Read More

Marie-Claire Diehl, BA
Read More

Shane Wright, BS
Read More
Diagnostic Screening & Comprehensive Psychological Evaluations

The Rochester Center for Behavioral Medicine is committed to an accurate diagnosis. We believe that before appropriate treatment (medication, psychotherapy, nutrition therapy) can be implemented, it is imperative to identify the extent and severity of your mental health condition.
Central to our approach is diagnostic screening, which plays a crucial role in this process. To enhance your care, we proudly present MindMetrix, an innovative protocol that harnesses industry-leading, peer-reviewed psychiatric rating scales. MindMetrix is expertly crafted to identify increased probabilities for over 60 mental health conditions. By screening for symptoms associated with these psychiatric conditions, we ensure that no co-occurring symptoms or conditions go overlooked. Best of all, this screening is conducted entirely online, allowing you to engage in the process from the comfort and privacy of your own home.
In addition to our diagnostic screening services, RCBM offers comprehensive psychological evaluations and testing for a variety of conditions, including Specific Learning Disorders in Reading, Mathematics, and/or Writing (previously known as Dyslexia, Dyscalculia, or Dysgraphia), Intellectual Disabilities, Autism Spectrum Disorder, Guardianship Evaluations, and High-Stakes Exam Accommodations Evaluations (such as ACT, SAT, LSAT, MCAT). We believe in working closely with patients, their families, and schools or employers to provide meaningful support following evaluations. Evaluations are conducted face-to-face at our welcoming office.
What is the difference between diagnostic screening and a comprehensive psychological evaluation?
- RCBM’s Diagnostic Screening is the first step toward a full psychological/psychoeducational evaluation. It provides some of the required documentation for Specific Learning Disabilities, Intellectual Disorder, and Autism Spectrum Disorder and it helps ensure that a full evaluation is necessary.
- In other words, Diagnostic Screening can rule out these conditions, but it is insufficient to diagnose (or confirm) these conditions are present for you.
- The results from your diagnostic screening will be reviewed at your results appointment by your licensed mental health clinician. If further evaluation is warranted for one of these conditions, the screening data will be used in conjunction with a full evaluation conducted by one of our licensed psychologists.
- Additional assessments that are completed through the Comprehensive Evaluation process, may be necessary to meet the accommodation requirements set forth by the organization that you are requesting accommodations at, such as your college or university.
- Psychological Evaluations are NOT billable to any insurance.
Watch: Expert Insights on Diagnostic Screening & Comprehensive Psychological Evaluations

Compass Program at RCBM
Alyssa Cooley, MA, Screening Team Clinical Lead, gives an overview of the COMPASS program at RCBM (Comprehensive Psychological Assessment & Screening Services). The program begins with diagnostic screening of up to 60 psychiatric conditions whose results help patients understand their mental health symptoms, clarify the overall clinical picture, and provide a strong foundation and support needed. If more specific information is needed to understand a learning disorder, cognitive changes, or ASD, a comprehensive psychological evaluation will be recommended to provide further clarification. The COMPASS program provides an overall personalized roadmap to arm patients with confidence and offer the right level of care.Eating Disorders


RCBM offers personalized, compassionate care for eating disorders treatment in Michigan and provides help for those suffering from all types of eating disorders and disordered eating. In addition, we have a Certified International Association of Eating Disorders (iaedp) Specialist on staff, along with other highly trained specialists in eating disorder treatment. You can rest assured knowing that we are deeply invested in assisting you or your loved ones on the road to recovery. There are many different types of eating disorders. Eating disorders are generally defined as a persistent disturbance in eating behaviors that impairs health or psychosocial functioning.
At RCBM, we work collaboratively as a team of prescribers, therapists, and registered dietitians. Eating disorder recovery is a journey, and therefore, we are dedicated to providing a holistic approach to treatment that addresses the physical, psychological, nutritional, and social aspects of eating disorders, including food and body image issues. We ultimately support you in achieving the life you want to live.
What Types of Eating Disorders Do We Treat?
We support individuals facing a range of eating disorders, including:
- Anorexia Nervosa
- Bulimia Nervosa
- Binge Eating Disorder
- Other Specified Feeding or Eating Disorders (OSFED)
- Avoidant/Restrictive Food Intake Disorder (ARFID)
Our Approach to Eating Disorder Therapy
Our care team includes psychiatrists, psychotherapists, and registered dietitians who work collaboratively to:
- Address underlying mental health conditions such as anxiety and depression
- Restore physical health through personalized nutrition
- Support long-term recovery using evidence-based therapies like CBT, DBT and mindfulness-based therapies
Why Choose RCBM for Eating Disorder Support?
With over 30 years of experience, RCBM offers a uniquely integrated approach that prioritizes:
- Mental health as part of physical recovery
- Trauma-informed, compassionate care
- Personalized treatment planning
Inner Door Center® Eating Disorders Treatment Program
RCBM and its medical director, Joel Young, MD, are proud to carry on the legacy and offer the Inner Door Center®'s Eating Disorders Treatment Program. The Inner Door Center® continues to be a dedicated program to improving the quality of life experience for our patients and promoting patient-centered care through evidence-based treatment, measurable outcomes, and team collaboration between disciplines.
FAQs
What is an eating disorder?
An eating disorder is a mental health condition defined by irregular eating behaviors that negatively impact one’s physical and mental well-being.
Some facts about eating disorders:
- Eating disorders are increasing among diverse ethnic and sociocultural communities despite beliefs that this only affects underweight, white females.
- Eating disorder behaviors in individuals who are over-concerned with body image are a physical manifestation of severe inner struggle.
- Eating disorders affect over 30 million people in the United States.
- Eating disorders are coping mechanisms that individuals have created to manage difficult experiences or feelings.
- Eating disorders frequently coexist with other psychiatric disorders, such as depression, substance use, OCD, PTSD, ADHD, or anxiety disorders.
- Eating disorders have the second highest mortality of any psychiatric diagnosis following opiate addiction.
In addition, there is much confusion about eating disorders and obesity. Obesity is not an eating disorder. Eating disorders are complex bio/psycho/social disorders that can do incredible harm and can be fatal and do not share the same way they are diagnosed and treated.
Share Link: What is an eating disorder?
How do I know if I have an eating disorder?
The SCOFF questionnaire is a valid and reliable five-question screening measure that assesses the probability that you are struggling with an eating disorder. It was developed by Morgan and colleagues in 1999.
SCOFF stands for Sick, Control, One, Fat, Food. Answering "yes" to two or more of the following questions indicates you may have anorexia nervosa, bulimia nervosa, or other eating disorders. Take the screening now:
- Do you make yourself Sick (induce vomiting) because you feel uncomfortably full?
- Do you worry you have lost Control over how much you eat?
- Have you recently lost more than One stone [approximately fifteen pounds] in a 3-month period?
- Do you believe yourself to be Fat when others say you are too thin?
- Would you say that Food dominates your life?
If you answered "yes" to two or more of the questions above, schedule an assessment with one of our registered dietitians. Our integrative approach involves a registered dietitian, a therapist, a physician, a nurse practitioner, or a physician assistant. Our treatment team and diagnostic testing can diagnose an accurate eating disorder and comprehensive care plan.
If you answered "no" to two or more questions but believe you may have a problem, if a loved one is concerned about your eating or exercise behavior, or if you are experiencing body image concerns, you should still seek help. The SCOFF questionnaire may not pick up all eating disorders or disordered eating behaviors, so it is important to consult with our treatment team to get help if you are struggling in silence.
Share Link: How do I know if I have an eating disorder?
What are the signs and symptoms of the different types of eating disorders?
The signs and symptoms of eating disorders vary for each person and depend on the type.
Anorexia Nervosa
Anorexia is a type of eating disorder characterized by extreme weight loss, excessive exercise, and severe restriction of food intake, leading to starvation. People with anorexia often have a distorted body image and are constantly driven to lose weight, feeling they're never thin enough. This obsession with weight loss and dieting can lead to serious health issues.
Bulimia Nervosa
Bulimia is an eating disorder characterized by cycles of binge eating followed by purging. This harmful pattern of indulgence and self-loathing can cause serious physical damage and requires prompt treatment. The desire to maintain a certain weight and body image often drives the cycle of losing control over food. Like anorexia, bulimia can lead to severe medical complications.
Binge Eating Disorder
Binge eating disorder is the most common type of eating disorder in the United States. BED affects an estimated 2.8 million people in the United States, according to a national survey. Binge eating is an eating disorder characterized by episodes of extreme overeating in a short period, leading to loss of control, followed by feelings of distress, guilt, shame, or disgust. It differs from overeating since it involves a lack of control and emotional turmoil. Binge eating disorder is a restrictive disorder that is not solved by more restriction through weight loss methods. Binge eating often serves as a coping mechanism for stress, anxiety, or depression.
Other Specified Feeding or Eating Disorders (OSFED)
Individuals with Other Specified Feeding or Eating Disorders (OSFED) often display disordered eating behaviors, distorted body image, and intense fear of gaining weight. OSFED is the most commonly diagnosed eating disorder among both adults and adolescents, affecting both males and females. Examples of OSFED include Bulimia Nervosa or Binge Eating Disorder with low frequency or limited duration; Atypical Anorexia Nervosa, where individuals exhibit restrictive behaviors but do not meet low weight criteria; Purging Disorder characterized by recurrent purging without binge eating, and Night Eating Syndrome involving recurrent episodes of eating during the night not explained by other factors. Individuals with OSFED have the same serious health risk factors as all other eating disorders.
Avoidant Food Intake Restrictive Disorder (ARFID)
Avoidant/Restrictive Food Intake Disorder (ARFID) doesn't involve distress about body shape or size, unlike other eating disorders. It can affect both children and adults. While picky eating is common in childhood, ARFID goes beyond normal pickiness, leading to inadequate calorie intake for proper growth and development in children and basic bodily functions in adults. ARFID can cause difficulties at school or work due to challenges eating with others and extended meal times. Symptoms may include a lack of interest in food, avoidance based on food's sensory characteristics, and concern about the negative consequences of eating, resulting in persistent failure to meet nutritional needs and compromised physical health.
Share Link: What are the signs and symptoms of the different types of eating disorders?
What are the underlying factors that lead to eating disorders?
Genetics/Biology:
- Eating disorders can run in families. Genetic factors may make you more susceptible to experiencing an eating disorder.
- Biological factors such as neurotransmitter imbalances, hormonal irregularities, and abnormalities in brain structure can contribute to the development of eating disorders.
- Often, an eating disorder develops as a result of a diet.
- If an individual has a family history of an eating disorder and never embarks on a weight loss diet, they then have a protection factor.
- If an individual has a family history of an eating disorder and embarks on a weight loss diet, this activates the reward pathway, like drug and alcohol addiction.
- A reward pathway, or reward system, refers to a group of brain structures that are activated by rewarding stimuli.
- The brain's most crucial reward pathway is the mesolimbic dopamine system. Though there are other existing reward pathways, the dopamine reward system is a key detector of rewarding stimuli.
- In this way, eating disorders may be classified as an addiction.
Cultural/Environment (Media):
- Sociocultural factors, including media portrayal of unrealistic body ideals, contribute significantly to the development of eating disorders.
- Pressure from peers, societal expectations, and cultural norms regarding body image can also play a role.
Triggers:
- Triggers for eating disorders vary widely and can include traumatic events, stress, major life changes, relationship issues, and societal pressures.
- Triggers can exacerbate underlying genetic predispositions and contribute to the onset or worsening of eating disorder symptoms.
Other Mental Health Issues:
- Eating disorders often co-occur with other mental health conditions, such as depression, anxiety disorders, ADHD, trauma, obsessive-compulsive disorder (OCD), and substance abuse.
- These comorbidities can complicate diagnosis and treatment, making it essential for healthcare providers to assess and address all underlying mental health issues.
- In addition, at least 30% of individuals diagnosed with an eating disorder have experienced trauma in their lives.
Overall, understanding the interplay between genetics/biology, cultural/environmental influences, triggers, and comorbid mental health conditions is crucial for effectively preventing, diagnosing, and treating eating disorders.
Share Link: What are the underlying factors that lead to eating disorders?
How do eating disorders mirror addictions?
The relationship between eating disorders and addiction is complex and multifaceted. While they are distinct conditions, they can co-occur and share some similarities regarding underlying physiological and psychological processes and behaviors.
Whether it is restricting, bingeing, purging, dieting, or any means to lose weight (compulsive exercise, weight loss medications), similar patterns of neural activation in someone with an eating disorder are also implicated in addictive-like behavior and substance dependence:
- Elevated activation in reward circuitry in response to food cues and behaviors such as restricting, bingeing, and purging.
- Reduced activation of inhibitory regions (hippocampus and insula) in response to food intake and other eating disorder behaviors
- Dopamine and endogenous opiates released.
- The individual may continue to crave the “high” from flooding the nucleus accumbens with behaviors.
Binge-eating and using addictive substances, such as alcohol and drugs, are working through the same neurotransmitter systems and regions in the brain. Sugar and dopamine-enhancing stimulant drugs (e.g., cocaine or amphetamine) show strong similarities in their motivational mechanisms. Attempts to treat binge eating using pharmacological interventions have demonstrated further similarities and relationships in the addictive process.
Share Link: How do eating disorders mirror addictions?
How do we treat eating disorders?
Addressing the underlying issues is crucial for recovery, along with normalizing eating patterns. The treatment for eating disorders typically involves a combination of medical, nutritional, and psychological interventions. Here are some common approaches:
Medical Monitoring: Initially, it's important to address any physical complications caused by the eating disorder, such as electrolyte imbalances, heart irregularities, or organ damage. Medical professionals may monitor vital signs, conduct blood tests, and address immediate health concerns.
Nutrition Counseling: Registered dietitians can help individuals develop healthy eating habits and meal plans. They work to restore proper nutrition and normalize eating patterns.
Therapy: Various types of therapy, such as cognitive-behavioral therapy (CBT) or dialectical behavior therapy (DBT), are often used to address the psychological aspects of eating disorders. Therapy helps individuals explore the underlying issues contributing to the disorder, develop coping strategies, challenge distorted thoughts about food and body image, and improve self-esteem.
Medication: In some cases, medication may be prescribed to address co-existing conditions such as depression, anxiety, or obsessive-compulsive disorder (OCD) that often accompany eating disorders. However, medication alone is usually not sufficient for treating eating disorders and is typically used as an adjunct to therapy.
Support Groups: Participating in support groups or group therapy sessions can provide individuals with a sense of community, understanding, and encouragement. It allows them to connect with others who are going through similar experiences and share coping strategies.
Family-Based Treatment (FBT): Particularly for adolescents with eating disorders, FBT involves the family as an integral part of the treatment process. It focuses on empowering parents or significant others to take an active role in their loved one’s recovery and restoring healthy eating habits within the family.
Holistic Approaches: Some individuals benefit from holistic approaches, such as yoga, mindfulness practices, art therapy, or acupuncture, as a complement to traditional treatment methods.
Hospitalization or Residential Treatment: In severe cases where there's a risk of serious medical complications or when outpatient treatment isn't effective, hospitalization or residential treatment programs may be necessary. These programs are available for all eating disorders across the spectrum, along with co-occurring disorders. These programs provide intensive medical and psychological support in a controlled environment.
SPRAVATO® (esketamine) Treatment: Spravato has demonstrated potential in the treatment of eating disorders, particularly for individuals with treatment-resistant eating disorders. Several clinical trials have been conducted to evaluate the effectiveness of Spravato in the treatment of eating disorders. One study published in JAMA Psychiatry found that Spravato was effective in reducing symptoms of depression and anxiety in individuals with treatment-resistant depression and comorbid eating disorders. Another study published in the Journal of Clinical Psychopharmacology found that Spravato was effective in reducing binge eating episodes and improving overall eating disorder symptoms in individuals with binge eating disorder.
Overall, the treatment plan should be tailored to the individual's needs, considering factors such as the type and severity of the eating disorder, coexisting conditions, and personal preferences. Treatment needs to be comprehensive, addressing both the physical and psychological aspects of the disorder, and for individuals to receive ongoing support throughout their recovery journey.
For more information on the treatment of eating disorders, refer to The American Psychiatric Association Practice Guideline for the Treatment of Patients With Eating Disorders.
Share Link: How do we treat eating disorders?
How effective is eating disorders treatment at RCBM?
At RCBM, we offer a multidisciplinary approach that includes medication prescribers, therapists, and dietitians, all crucial team members in treating eating disorders. Prescribers can monitor physical health, address medical complications, and provide necessary medications. Therapists offer psychological support, help patients explore underlying issues, and develop coping strategies. Dietitians provide nutritional guidance, help normalize eating patterns, and support patients in establishing a healthy relationship with food. This collaborative approach and the evidence-based interventions listed below ensure comprehensive care, address various aspects of the disorder, and increase the likelihood of successful treatment outcomes.
Anorexia Nervosa:
The treatment of Anorexia nervosa, like other eating disorders, requires a team approach. The first treatment priority is establishing a consistent eating routine to prevent long-term health complications. Individuals are provided the necessary support to establish a healthy weight for their body that ensures a regular menstrual cycle, sufficient cardiac health, adequate energy levels, and normal lab values. Many tests are completed by a physician to rule out other factors that may be contributing to weight loss and/or loss of appetite and to ensure immediate health concerns are addressed. A dietitian works with the individual to safely increase intake, address nutritional deficiencies, and ensure adequate intake. Many individuals utilize restrictive behaviors to cope with life’s challenges and to create a false sense of control. Therapists can work with individuals to make these connections and identify healthy alternative coping mechanisms. Compensatory behaviors, obsessive thoughts about food and dieting, and concerns about body image are also addressed by the care team. Meal support to provide accountability and alleviate anxiety with foods may also be incorporated into the treatment plan. Depending on the age and needs of the individual, family-based treatment may also be integrated.
Bulimia Nervosa:
Bulimia nervosa treatment is similar to anorexia nervosa, with an emphasis on providing education about the negative long-term effects of compensatory behaviors. Lessening behaviors such as intentional vomiting, laxative use, and/or compensatory exercise is a treatment priority. The treatment team will work with the individual to identify triggers for these behaviors and develop healthy alternative coping mechanisms to replace compensatory behaviors.
Binge Eating Disorder:
Addressing the underlying issues of binge eating disorder is crucial for recovery. Still, treatment does not focus on weight loss, as this can exacerbate the disorder and underlying trauma as childhood trauma factors into up to 75% of individuals with BED. A total of 60% of people with BED have been diagnosed with complex PTSD. In turn, a weight loss regimen is another form of trauma to the body.
Normalizing eating patterns is key to managing binge eating disorder and can help achieve overall health goals. Binge eating disorder is a restrictive disorder that is not solved by more restriction through weight loss methods.
Individuals feel extreme shame and confusion about binge eating. They have tried to stop many times on their own, including dieting, and their inability to control this behavior is a source of deep embarrassment. When treatment focuses on helping individuals understand that binge eating develops principally as an adaptation to complex trauma as a means of self-protection and from the deprivation created by dieting, self-compassion begins to develop.
Binge eating is a survival tool that develops when little else is available. As a result, changing the behavior is often terrifying. Breaking the cycle can feel impossible, not because individuals are weak or lack willpower, but because they are trying to change a protection they have relied on for a long time. Once an individual can understand the reasons binge eating may be protective for them, their shame about going to food to cope can decrease.
Dieting to combat binge eating disorder is futile and dangerous, setting one’s self up for a cascade of events as described above.
OSFED
We take all other eating disorders seriously. Depending on how this eating disorder's diagnosis presents itself, this will guide the treatment using interventions used in anorexia nervosa, bulimia nervosa, and binge eating disorder.
ARFID
Avoidant Restrictive Food Intake Disorder treatment involves a thorough assessment to determine if food aversion and/or fear of choking or allergic reaction are present. Registered dietitians assess for nutritional deficiencies and adequate intake.Therapists work with individuals to improve distress tolerance with food exposures.
Share Link: How effective is eating disorders treatment at RCBM?
Ready to get started in the eating disorders program at RCBM?
If you are a current patient at RCBM, don't hesitate to contact our office at (248) 608-8800. If you are new to RCBM, including stepping down from a higher level of care eating disorders treatment center, please complete the new patient registration form. Once you submit the form, we will match you with one of our qualified prescribers, therapists, and registered dietitians specializing in eating disorders treatment. If you are stepping down from a higher-level care treatment program, we will connect with your discharge team if you have a release of information on file with your respective treatment center.
Please note that individuals must be residents of Michigan. We are committed to helping you throughout your recovery journey and look forward to working with you.
Share Link: Ready to get started in the eating disorders program at RCBM?
Watch: Expert Insights on Eating Disorders


Treating Eating Disorders through Psychotherapy
Julia Rodgers, BSN, LLMSW explains how the treatment of eating disorders addresses psychological issues, relationship issues and life experiences that contribute to disordered eating. She provides strategies for dealing with uncomfortable emotions, patterns of thinking, along with untangling body image and expanding self-worth beyond an individual's physical body.
How to treat Eating Disorders with a Registered Dietitian
Chelsea Carpentier, RDN, MSN, discusses medical nutrition therapy for eating disorders. She explains the intake process involved to create a personal treatment plan that may include identifying and managing behaviors such as bingeing, purging, or restricting, along with building a healthy relationship with exercise, intuitive eating, and body neutrality concepts.
The Spravato Program at RCBM
Hailee Mika, Spravato Program Coordinator, discusses Spravato and how it helps treatment-resistant depression. She also explains how our program works at RCBM, from referral and authorization to the treatment experience. Note: As of February 2025, the FDA has approved Spravato as monotherapy for adults living with treatment-resistant depression (TRD).
Spravato Program at RCBM
Dr. Joel Young discusses the use of Spravato for treatment-resistant depression and how to enroll in our Spravato Program at RCBM.Meet the Providers Who Offer Care for Eating Disorders

Alicia Basin, MA, LPC
Read More

Alli Smith, LMSW, CCTP
Read More
Aundreah Walenski, LMSW
Read More

Beverly Price, RD, MA, CEDS-C, E200-RYT, C-IAYT
Read More
Brady Brower, PA-C
Read More
Bryn Thompson, PA-C
Read More

Chelsea Butler, RDN, MSN (formerly Carpentier)
Read More

Elizabeth Sweet, DNP, APRN, PMHNP-BC
Read More
Jennifer Lindsey, LMSW
Read More
Jennifer Stone, MA, LPC, NCC, CAADC
Read More

Jessica Grzybowski, RDN
Read More
Joel L. Young, MD, Medical Director and Founder
Read More
Kaca Popovic, MA, LPC
Read More

Katie Young, MSN, NP, PMHNP-BC
Read More
Kendra Ball, LMSW
Read More

Kimberly Roznowski, PA-C
Read More

Laurel Saint Cyr, PA-C
Read More
Lisa Michaux, MSN, PMHCNS-BC
Read More

Sarah Hutton, MD, Associate Medical Director
Read More
Sarah Krasnick, MSN, RN, ANP-C, PMHNP-BC
Read More

Sheri Strzelecki, MSN, FNP-BC, PMHNP-BC
Read More

Susha Panicker, MSN, PMHNP-BC, FNP-BC
Read More

Sydney Salloum, LPC
Read More
Related Titles from the RCBM Reading and App list:
Aging with Vitality and Body Liberation - By Debra Benfield, RDBeyond Beautiful: A Practical Guide to Being Happy, Confident, and You in a Looks-obsessed World - By Anuschka Rees
Body Kindness - By Rebecca Scritchfield, RDN
Health at Every Size: The Surprising Truth About Your Weight - By Linda Bacon
Making Weight: Healing Men’s Conflicts with Food, Weight, and Shape - By Arnold Andersen, M.D., Leigh Cohn M.A.T., Tom Holbrook, M.D.
More Than a Body: Your Body Is an Instrument, Not an Ornament - By Lexie Kite and Lindsay Kite
Sick Enough: A Guide to the Medical Complications of Eating Disorders - By Jennifer Gaudiani
Surviving an Eating Disorder: Strategies for Family and Friends - By Michelle Siegel, Judith Brisman, and Margot Weinshel
The Body Image Workbook: An Eight-Step Program for Learning to Like Your Looks - By Thomas Cash, PhD
The Body Image Workbook for Teens: Activities to Help Girls Develop a Healthy Body Image in an Image-Obsessed World - By Julia V. Taylor
The Body is Not an Apology and Your Body is Not an Apology Workbook - By Sonya Renee Taylor
The Longest Match: Rallying to Defeat an Eating Disorder in Midlife - By Betsy Brenner
The Parent’s Guide to Eating Disorders: Supporting Self-Esteem, Healthy Eating, and Positive Body Image at Home - By Marcia Herrin EdD, MPH, RD and Nancy Matsumoto
Using Writing as a Therapy for Eating Disorders: The Diary Healer - By June Alexander
Fibromyalgia and Chronic Fatigue Clinic
At RCBM, we understand that both fibromyalgia and chronic fatigue syndrome are complex, often misunderstood conditions that impact every part of daily life. Patients commonly report unrelenting fatigue, non-restorative sleep, migrating muscle aches, tension headaches, and cognitive difficulties like impaired short-term memory - often described as “fibro fog” or “brain fog.” These symptoms may stem from or overlap with myalgic encephalomyelitis (ME/CFS) or fibromyalgia.
If you've been struggling to find answers or relief, our team is here to help.
Dr. Joel Young, MD - Medical Director and Founder of RCBM - has developed a deep clinical interest in ME/CFS and fibromyalgia. He has led clinical studies on medication management and authored Understanding and Treating Chronic Fatigue: A Practical Guide for Patients, Families, and Practitioners (Praeger, 2020), which explores how to manage chronic fatigue, brain fog, chronic pain, and sleep disruption.
About the Program
The Rochester Center for Behavioral Medicine, located north of Detroit, is pleased to announce the launch of our Fibromyalgia and Chronic Fatigue Clinic, directed by Joel L. Young, MD. This specialized program is designed to help individuals struggling with fibromyalgia, chronic fatigue, and related somatic syndromes through evidence-based, centrally acting treatments.
Our Approach
Unlike procedure-oriented or interventional pain clinics, RCBM’s approach focuses on the neurobiological and behavioral aspects of fibromyalgia and chronic fatigue. Our clinicians utilize medications that target the central nervous system to help alleviate pain, mitigate fatigue, and enhance daily functioning.
We emphasize comprehensive, individualized care — combining pharmacologic treatment with behavioral and lifestyle interventions to address the complex interplay between mind and body.
Comprehensive, Multidisciplinary Care
Our program offers integrated therapeutic services designed to support both body and mind:
- Medication management focused on centrally acting, evidence-based treatments
- Individual therapy to help patients manage stress, mood, and coping strategies associated with chronic fatigue and fibromyalgia
- Expert dietitian support to address the nutritional factors that influence fatigue, energy, and inflammation
- Coordination of care for patients with fatigue associated with ADHD and related neuropsychiatric conditions
Why Choose RCBM
- Expert leadership under Joel L. Young, MD, a nationally recognized psychiatrist and researcher
- Collaborative, multidisciplinary team of psychiatric, therapy, and nutritional professionals
- Focus on centrally acting medications, not procedural interventions
- Integration of research-based knowledge into real-world patient care
- Commitment to helping patients reclaim energy, focus, and quality of life
What is Chronic Fatigue Syndrome (CFS)
Complaints of chronic fatigue are commonly expressed by individuals to their physicians and mental health therapists. Those who suffer from this debilitating condition feel continuous exhaustion and a feeling comparable to that of having just run a marathon when all they have done is a daily living task, such as taking a shower or getting dressed. Beyond chronic fatigue, individuals report trouble getting out of bed or feeling that sleep has not restored energy. Many describe migrating aches and pains, often conveyed as upper neck muscle tension and headaches. In addition to overwhelming exhaustion, most individuals with these symptoms also report an impaired short-term memory described as “brain fog.” These later symptoms are referred to as myalgic encephalomyelitis (ME). In addition, individuals with these symptoms often are told that their symptoms are “All in Your Head.”
It is estimated that between 1 million and 2.5 million people suffer from CFS. In 2015, the Centers for Disease Control and Prevention (CDC) published diagnostic criteria for ME/CFS based on those of the National Academy of Medicine. Often told that their complaints were phantom, the official recognition of ME/CFS as a real disease was viewed as a validating step toward recognition and better understanding of this medical problem.
What is Fibromyalgia?
Fibromyalgia is a chronic neurological condition that causes widespread pain and tenderness throughout the body. It affects how the nervous system processes pain signals, making the brain and spinal cord more sensitive to pain and other sensory stimuli. It is more common in women and often appears between ages 20 and 50, but can occur at any age. It frequently occurs alongside other chronic conditions such as arthritis, lupus, or chronic fatigue syndrome.
Key symptoms include:
- Widespread muscle and joint pain
- Fatigue and feeling exhausted even after sleep
- Sleep problems (non-restorative sleep, insomnia)
- Brain fog (difficulty with memory or concentration)
- Headaches or migraines
- Digestive issues such as IBS
- Sensitivity to noise, light, temperature, or touch
- Numbness or tingling in hands and feet
Although the exact cause isn’t fully known, research suggests it involves a combination of genetics, stress or traumatic events, and infections or illnesses that trigger symptoms and/or changes in how the brain processes pain.
FAQs
How do fibromyalgia and chronic fatigue differ?
CFS and fibromyalgia are classified as distinct conditions, yet they share many characteristics. Chronic fatigue is the primary complaint of an individual with CFS, whereas fibromyalgia is characterized by pain and stiffness throughout the body. The pain migrates throughout the body, with the upper neck and back most commonly involved. As with CFS, people with fibromyalgia often suffer from fatigue as well as brain fog, but the leading symptom is pain. Complicating the issue further, it is common to have both CFS and fibromyalgia.
About 4 million adults in the United States have fibromyalgia, and the risk increases with aging. Women are at twice the risk for fibromyalgia compared to men. In addition, people who have had lupus or rheumatoid arthritis have an elevated risk of developing fibromyalgia.
People with fibromyalgia may have difficulty with concentration, memory, and thinking (brain fog), and they may suffer from headaches and sleep problems. Most people with fibromyalgia are diagnosed in their middle age, although people of any age may be affected by these debilitating symptoms. There are two other distinctions between the two conditions. Some research supports the idea that physical exercise is helpful for fibromyalgia but may make CFS worse.
The FDA has approved several medications for the treatment of fibromyalgia. Pregabalin (Lyrica), duloxetine (Cymbalta), or milnacipran (Savella) all have adequate data studies showing their usefulness for fibromyalgia symptoms. These medications will help certain types of fibromyalgia pain, specifically neuropathy (nerve tingling) and sometimes muscle aches. It is important to note that they do not significantly help brain fog and other impairing cognitive symptoms common to fibromyalgia and CFS.
Share Link: How do fibromyalgia and chronic fatigue differ?
How does long COVID, ADHD and Lyme disease set the stage for chronic fatigue syndrome?
COVID
Post-COVID, chronic fatigue symptoms, and chronic fatigue syndrome are a very related phenomenon. The belief is that a minority of individuals with an acute COVID-19 infection will develop symptoms of chronic fatigue, often months after contracting coronavirus. These individuals progress to be ‘long-haulers’ with chronic fatigue, weakness, shortness of breath, and sometimes confusion.
LYME DISEASE
When Lyme disease is diagnosed in the early stages, the infection can be treated with certain antibiotics. Treatment may last from ten days to up to three weeks. Most people recover with treatment, but some people develop fatigue and muscle pain that can extend for up to six months. However, some individuals have chronic fatigue years after a tick bite, known as “Post-Treatment Lyme Disease Syndrome.”
ADHD
Many cases of CFS are the result of childhood ADHD. It is believed that brain fog results from the same biological process that causes ADHD, namely a complex dysregulation of the brain’s dopamine and norepinephrine modulation. Some researchers have found that the presence of ADHD, along with CFS and depression, increases the intensity of fatigue. It also is linked to an earlier age of onset of CFS. Researchers have found that individuals with ADHD had an earlier age of onset of chronic fatigue syndrome (age 30) than the subjects who did not have ADHD (35 years). Post-COVID, chronic fatigue symptoms, and chronic fatigue syndrome are closely related. It is believed that a small percentage of individuals who have had COVID-19 may develop symptoms of chronic fatigue months after contracting the virus. These people may become "long-haulers" with chronic fatigue, weakness, shortness of breath, and confusion.
Share Link: How does long COVID, ADHD and Lyme disease set the stage for chronic fatigue syndrome?
How is chronic fatigue syndrome and fibromyalgia treated at RCBM?
At RCBM, we provide integrated, collaborative care for CFS. We integrate medication management, psychotherapy, and medical nutrition therapy, which all work together to give you the relief you have been desperately seeking. RCBM has published three peer-reviewed papers examining the treatment of chronic fatigue, including fatigue associated with attention-deficit disorder.
Medication Management
Before medication is prescribed, you will undergo diagnostic screening to better understand your presenting issues. This will help customize your treatment plan with the appropriate medication management solution. Dr. Joel Young, MD, RCBM's medical director, is strongly interested in CFS and has published the book Understanding and Treating Chronic Fatigue: A Practical Guide for Patients, Families, and Practitioners. (Praeger, 2020). In addition to lifestyle modifications, pharmacologic treatments for individuals with CFS are presented that include the use of long-acting stimulants such as lisdexamphetamine (LDX) in the management of chronic fatigue, brain fog, chronic pain, and sleep problems associated with ME/CFS. Several FDA-approved medications are available for fibromyalgia. A new treatment option Tonmya— low-dose cyclobenzaprine — has recently received FDA approval and will become available in late November. Our clinic will be among the first in Michigan to incorporate this therapy into a broader treatment framework for fibromyalgia.
Psychotherapy
For individuals suffering from both CFS and fibromyalgia, psychotherapy is a meaningful addition to antidepressant medications. Individual psychotherapy is an approach in which all therapists at Rochester Center are highly trained. The connection of a patient to a thoughtful therapist can be powerful. Our therapists can explore your feelings about your condition and can help you identify and neutralize negative thought patterns.
RCBM also uses mind-body-focused therapy. Mind-body medicine focuses on the brain's connections to the body and how emotions, verbalizations, behaviors, and spirituality directly affect health and well-being. It is a cognitive-behavioral therapeutic practice that enhances awareness of thoughts and actions to improve self-esteem and self-confidence, and allows one to live the life one desires.
Medical Nutrition Therapy
Our registered dietitians will assess your diet and develop a personalized nutrition plan to alleviate your symptoms. A thorough assessment paves the way for a successful nutrition counseling experience. A review of food intake and behaviors, an evaluation of the meal plan, and further information are provided at follow-up appointments. Medical nutrition therapy is a crucial part of managing CFS and fibromyalgia, as certain foods can alleviate symptoms of CFS and fibromyalgia while other foods may exacerbate symptoms. Diet is an integral part of CFS and fibromyalgia management that should not be ignored.
Share Link: How is chronic fatigue syndrome and fibromyalgia treated at RCBM?
How effective is treatment of chronic fatigue syndrome and fibromyalgia at RCBM?
Medication Management
Joel Young, MD, RCBM's medical director and founder, has authored the book Understanding and Treating Chronic Fatigue: A Practical Guide for Patients, Families, and Practitioners. In it, he describes his work with long-acting stimulant medications that force many of the physical symptoms experienced in CFS into retreat. Treatment with lisdexamphetamine (LDX), a long-acting stimulant, was studied in the Clinical Trials Group at RCBM.
The participants in this study were between the ages of 21 and 59. All the subjects were female except for one. Two groups were randomly assigned: one group to the active agent (LDX) and the other half to a placebo. Over six weeks, global CFS symptoms respond favorably to LDX. Compared to a placebo, LDX improved cognitive deficits. In addition, subjects treated with LDX reported less fatigue and general anxiety, along with a significant decrease in physical pain.
Psychotherapy
Clients who participate in individual therapy work with their therapist to gain insight and increase coping skills to improve general mental health. In addition, individuals with CFS are prone to taking shallow, rapid breaths rather than slow, deep breaths. Regular meditation can help patients with CFS or fibromyalgia get into a more natural, healthy breathing rhythm while feeling a sense of peace and calm. This practice, along with the other techniques discussed above, will enhance your mental and physical health. Several clinical studies indicate that integrative therapies can help patients cope and manage pain, minimize stress and anxiety, and gain an overall sense of control over their mind and body.
Medical Nutrition Therapy
Clinical improvements in CFS and fibromyalgia were observed after following various diets, including a diet rich in antioxidants (e.g., plant-based and Mediterranean-style diets), a low FODMAP diet, a gluten-free diet, or an anti-inflammatory diet (gluten-free, with elimination of sugar, dairy, and processed foods).
An unhealthy gut microbiota can affect macronutrient digestion and the absorption of minerals and vitamins. A lack of beneficial bacteria can alter the production of gut microbiota metabolites, such as SCFAs (e.g., butyrate) and secondary bile acids. This can affect gut sensitivity, permeability, and immune response, contributing to low-grade inflammation.
Essential fatty acids are found in several foods: meats and dairy products, fish and seafood, whole grains, fruits, and vegetables. The amount of essential fatty acids in meat and dairy products is reasonably small compared to the total fat (especially saturated fat) in these foods. In contrast, omega-6 fatty acids, through their conversion in the body to other substrates, are implicated in autoimmune diseases such as chronic fatigue syndrome, rheumatoid arthritis, psoriasis, inflammatory bowel disease, and asthma.
Share Link: How effective is treatment of chronic fatigue syndrome and fibromyalgia at RCBM?
Dr. Young’s publications and presentations on chronic fatigue syndrome
Scientific Reviewer, Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Panel for Department of Defense’s Congressionally Directed Medical Research Programs, May 2023 - present.
Chair, Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (CT-ME/CFS) Peer Review Panel, Peer Reviewed Medical Research Program (PRMRP) for the Department of Defense (DOD) Congressionally Directed Medical Research Programs (CDMRP), October 2021.
Chronic fatigue syndrome: 3 cases and a discussion of the natural history of attention-deficit/hyperactivity disorder. Postgraduate Medicine, January 2013.
“Use of lisdexamfetamine dimesylate in treatment of executive functioning deficits and chronic fatigue syndrome: A double-blind, placebo-controlled study.” Psychiatry Research, October 2012.
Poster presentation at 2012 American Psychiatric Association Conference, May 7, 2012. Poster #34399.
“ADHD is a notable characteristic of patients suffering from chronic Lyme disease: a survey of adults at the Michigan Lyme Disease Association Conference.” Poster presentation at 2011 U.S. Psych and Mental Health Congress, November 8, 2011. Poster # 111.
Poster presentation at 2011 U.S. Psych and Mental Health Congress, November 8, 2011. Poster # 110.
Use of lisdexamfetamine dimesylate in treatment of cognitive impairment and fatigue (Chronic Fatigue Syndrome): A double-blind, placebo-controlled study, November 2011.
Primary Investigator: RCBM: Use of Lisdexamfetamine Dimesylate in the Treatment of Cognitive Impairment (Chronic Fatigue Syndrome): A Double-Blind, Placebo-Controlled Study, September 2009.
“AD/HD: Is There a Link to Fibromyalgia, Chronic Fatigue Syndrome, and Other Pain Issues?” Michael Golds Conference: Oakland Community College, Farmington Hills, MI, October 2006.
Share Link: Dr. Young’s publications and presentations on chronic fatigue syndrome
How do I get started in the fibromyalgia and chronic fatigue clinic at RCBM?
If you are a current patient at RCBM, please contact our office at (248) 608-8800. If it has been more than three years since you have had diagnostic screening, we will need to re-administer before treatment. If you are new to RCBM, please complete our new patient registration form to start the admission process.
Individuals must reside in the state of Michigan and be willing to come to the office if needed.
We look forward to helping you feel better!
Share Link: How do I get started in the fibromyalgia and chronic fatigue clinic at RCBM?
The following articles on our blog offer additional information on Chronic Fatigue Syndrome
Can chronic fatigue syndrome be treated? Rochester-based doctor is trying to find an answer
Rochester area doctor studying treatment for chronic fatigue found linked to COVID-19
New Hope for Chronic Fatigue Sufferers
Chronic Fatigue Syndrome IS Real
Watch: Expert Insights on Fibromyalgia and Chronic Fatigue Clinic

Chronic Fatigue in COVID Long Haulers
Joel Young, MD, Medical Director RCBM discusses chronic fatigue in COVID long haulers.
Chronic Fatigue Syndrome
Dr. Young is interviewed on WXYZ-TV Channel 7, with Andrea Isom, with this heartfelt story on chronic fatigue, RCBM's research, and a treatment that's working for patients.
Metro Detroit woman shares her battle with chronic fatigue syndrome
Melanie Lusnak shares her battle with chronic fatigue syndrome and the help she received from Dr. Joel Young that changed her life.
Chronic fatigue syndrome and long term effect of COVID-19
Chronic fatigue syndrome is a common disorder affecting at least 2.5 million Americans nationwide, including many COVID-19 patients. Dr. Young shared his research and new hope for people like Melanie, a local woman who has improved with treatment. Watch his interview on Fox 2 TV Detroit.
Chronic Fatique Syndrome
Joel Young, MD discusses new treatments for chronic fatigue syndrome and discusses similarities and differences between chronic fatigue syndrome and fibromyalgia.Meet the Providers Who Offer Care for Fibromyalgia and Chronic Fatigue Clinic
Joel L. Young, MD, Medical Director and Founder
Read More
Beverly Price, RD, MA, CEDS-C, E200-RYT, C-IAYT
Read More

Melissa Oleshansky, PhD, LP, RYT
Read More
Related Titles from the RCBM Reading and App list:
Understanding and Treating Chronic Fatigue: A Practical Guide for Patients, Families, and Practitioners - By Joel Young, MDGrief/Loss/Coping with Illness Issues

Sudden loss of a loved one from a heart attack, stroke, homicide, suicide or accident, often presents many issues for those left behind. People who experience loss from divorce, chronic or terminal illness face a different type of grieving. There are also differences in how adults, children, men and women experience grief and loss.
RCBM clinicians are well-trained in helping individuals through the grieving process, whether grieving the loss of a loved one or coping with their own terminal illness. Some of the therapeutic interventions used at RCBM include techniques in relaxation, cognitive restructuring, stress management, goal setting, learning new coping skills, improving communication skills with loved ones as well as with medical personnel, and referral to community support groups. Each case is looked at individually and the type of loss is taken into consideration when a treatment plan is created. RCBM also offers the services of our Psychiatrist and Nurse Practitioners who can evaluate patients who may need medication as an adjunct to their therapy.
Related Titles from the RCBM Reading and App list:
A Mother Loss Workbook: Healing Exercises for Daughters - By Diane HambrookBeing Mortal - By Atul Gawande
Growing up Motherless - By Lynn Davidman
How to go on Living When Someone You Love Dies - By Therese A. Rando
How to Survive the Loss of a Parent: A Guide for Adults - By Lois Akner
Motherless Daughters - By Hope Edelman
On Grief and Grieving - By Elisabeth Kubler-Ross and David Kessler
Proof of Heaven - By Eben Alexander
The Grief Recovery Handbook: The Action Program for Moving Beyond Death, Divorce, and Other Losses - By John James and Russel Friedman
The Orphaned Adult: Understanding & Coping with Grief & Change After the Death of Our Parents - By Alexander Levy
Under the Whispering Door - By TJ Klune
Wait until next year - By Doris Goodwin
When Breath Becomes Air - By Paul Galanithi
Individual Therapy

Individual psychotherapy is an approach in which all therapists at Rochester Center are highly trained. Individuals receive assistance in addressing issues related to self, family, school and work. Clients who chose to participate in individual therapy work together with their therapist to gain insight and increase coping skills in order to improve general mental health.
At the Rochester Center for Behavioral Medicine (RCBM) therapists work closely with the Psychiatrists, Physician Assistants, Nurse Practitioners, and if your case involves our Registered Dietitian, in a therapeutic team approach. This provides a broader viewpoint of existing mental health issues. When deemed necessary by the mental health professionals at RCBM, psychiatric evaluations, medication management, and medical nutrition therapy, along with family or marital counseling may be recommended.
The professionals at RCBM also encourage clients to take an active role in participating in their therapy. Therapists may also provide psychoeducation through the use of videos, bibliotherapy, and opportunities to attend seminars pertaining to individual mental health issues. Please view our Professionals page to view the backgrounds and related interests of a particular therapist at RCBM.
Watch: Expert Insights on Individual Therapy
What is Cognitive Behavioral Therapy (CBT)?
Dr. Melissa Oleshansky, PhD discusses cognitive behavioral therapy (CBT). This structured and goal-oriented psychotherapy is used at RCBM to treat or manage mental health conditions, stress, unhealthy habits, and emotional concerns.
What is Dialectical Behavioral Therapy?
Aundreah Walenski, LMSW discusses the components of dialectical behavioral therapy (DBT), an evidence-based psychotherapy that is used to treat personality disorders and interpersonal conflicts and how this modality can help individuals live the life they want to live.
How to Talk to a Loved One About Psychiatric Treatment
Jamie Clark, LMSW explains the best way to discuss mental healthcare with your loved one including finding a safe, comfortable and private place to express how each of you feel. It's imperative to stress the importance of not only physical but mental health care along with assisting your loved one in finding resources.
What Should a Patient Know Before Starting an Antidepressant
Chris Discenna, PA-C sets your expectations for starting antidepressant medication, including not to expect immediate improvement as medications take time to work, side effects you may experience and how to manage, along with the possibility of you needing a dose adjustment or a different antidepressant agent. Combining medication with therapy is highly recommended for a more comprehensive approach for long term outcomes.
Feeling Stuck in Therapy? Here’s What to Do Next
Melissa Oleshansky, PhD, "Dr. O", explains that feeling "stuck" in therapy is not failure, but that you are on the right edge of meaningful change. Dr. O highlights three strategies to go deeper in therapy including "saying what you are not saying", "get curious not critical", and "change the rhythm not the song". Therapy is an evolving process. It requires you to "lean in." "Stuckness" is not a problem but a portal to something deeper.
Mental Health First Aid
Maegan Wickstrom, LMSW explains mental first aid which is an evidence-based training that teaches mental health professionals to respond to a challenge or crisis appropriately. As a therapist trained in mental health first aid, Maegan is trained to provide supportive intervention and education to patients and family members, along with tools and strategies for their current situation. Mental health first aid helps patients feel more prepared when struggling by supporting, listening, validating and connecting the individual to appropriate resources vs. just fixing the issue.
Family Member with Depression
Kelly Dahl, LMSW describes the challenges that family members or caregivers face when supporting someone with depression. They may feel overwhelmed and unsure of how to support, but it's important for them to be there without trying to fix the problem. Strategies and resources include listening with empathy, not trying to find a solution, and connecting. They don't have to completely understand but leave it to the professionals to do the "heavier lifting." Family members and caregivers can advocate for their loved one by going with them to their appointments, or help them set up simple routines including eating, sleeping, self-care or joining them on a walk.
Emergency Responder Training
Jamie Fulton-Smith, MS, LLP, ERPSCC, describes her training as an emergency responder, public safety certified clinician. Her training involved over 40 hours of continuing education and passage of an examination in a year-long program from the National Emergency and Public Safety Center in Colorado. The training addressed the unique stressors first responders face, relationships and family dynamics, resiliency, suicide prevention, and post critical incident response. Her training has helped her support first responders as they navigate the pressures of a dangerous and high-demand career, while suffering from higher rates of morbidity, premature deaths, depression, PTSD, and suicidality than the general population. Although stigma remains, with responders reluctant to seek treatment, certified providers such as Jamie can help break down barriers and improve mental health outcomes for this population.Related Titles from the RCBM Reading and App list:
Atomic Habits: An Easy and Proven Way to Build Good Habits and Break Bad Ones - By James ClearDBT Skills Training Handouts and Worksheets Second Edition - By Marsha M. Linehan
Dialectical Behavior Therapy Skills Training with Adolescents: A Practical Workbook for Therapists, Teens, and Parents - By Jean Eich
Feeling Great: The Revolutionary New Treatment for Depression and Anxiety - By David Burns
Reclaim Your Life: Acceptance and Commitment Therapy in 7 weeks - By Carissa Gustafson
The Dialectical Behavior Therapy Skills Workbook - By Matthew McKay, Jeffrey Wood, and Jeffrey Brantley
The DBT Deck for Clients and Therapists: 101 Mindful Practices to Manage Distress, Regulate Emotions, and Build Better Relationships - By Lane Pederson
CPT Coach
PE Coach
Medical Nutrition Therapy

At RCBM, we offer medical nutrition therapy (MNT) by registered dietitians. How are eating habits and mental health care related? MNT is an essential adjunct to enhancing mental well-being and an important component of physical health. It is based on decades of medical research on the relationship between diet, nutrition, and health outcomes. The process includes a food and behavior assessment, health and treatment history, interface with other providers, and meal and treatment planning. A thorough assessment paves the way for a successful nutrition counseling experience. At follow-up appointments, food intake and behaviors are reviewed, the meal plan is evaluated, laboratory results are reviewed, and further information is provided.
New: Register for our Nutrition Webinar
What is Medical Nutrition Therapy (MNT)?
- MNT is an individualized approach that blends medical and nutritional guidance to support mental health and well-being.
- It’s not about dieting - it’s about supporting emotional health, physical health, and balanced nutrition.
- At RCBM, our registered dietitians provide Medical Nutrition Therapy to help patients build a healthier relationship with food, focusing on how nutrition impacts mood, focus, and emotional well-being.
Who Can Benefit from Medical Nutrition Therapy?
- Individuals with eating disorders or disordered eating, including ARFID
- Those experiencing anxiety, depression, chronic fatigue or ADHD that impacts eating
- Medical concerns such as diabetes, PCOS, cardiovascular disease, gastrointestinal disorders
- Patients navigating weight changes or medication-related appetite shifts
- Anyone seeking to build a more balanced, intuitive approach to nutrition
How Does Medical Nutrition Therapy Work at RCBM?
- Initial comprehensive assessment
- Collaborative treatment plan
- Ongoing support tailored to personal goals and medical needs
What to Expect During Your Sessions
- Goal-setting and personalized meal planning
- Understanding how nutrition impacts mood and focus
- Addressing food fears, body image concerns, or emotional eating
- Support for nutrition challenges linked to medications or mental health conditions
FAQs
What is the difference between Medical Nutrition Therapy and general nutrition advice?
Medical nutrition therapy (MNT) is a specialized treatment provided by registered dietitians (RD) to manage specific medical conditions through tailored nutrition plans. MNT involves a comprehensive assessment and ongoing support to monitor progress. Registered Dietitian Nutritionists (RD/RDN) are food and nutrition experts who have met the Commission on Dietetic Registration (CDR) criteria to earn the RD credential. This includes:
- A Bachelor of Science degree and a Master's degree.
- The curriculum is weighted heavily in the sciences (chemistry, biochemistry, physiology, pharmacology), and students are prepared to apply to medical school should they choose.
- 1000 supervised hours of a post-baccalaureate internship.
- Learning Activities and Competency Evaluation set forth by the Accreditation Council for Education in Nutrition and Dietetics (ACEND), the accrediting agency for education programs that prepare students for careers as registered dietitians, following successfully passing their board examination.
General nutrition advice focuses on basic dietary guidelines for healthy eating without addressing specific health issues. It is less personalized and does not typically require medical oversight. Nutrition advice may come from individuals with titles such as “health coach” or “nutrition consultant. " They are not subject to the same intensive training or education as a registered dietitian, and their advice may be harmful.
Share Link: What is the difference between Medical Nutrition Therapy and general nutrition advice?
Can Medical Nutrition Therapy help with emotional eating and stress?
Medical Nutrition Therapy (MNT) can be a valuable tool for addressing emotional eating and stress by combining clinical nutrition expertise with personalized behavioral strategies.
Here are a few strategies our registered dietitians offer to support patients. Our registered dietitians can help you:
- Identify the emotional, psychological, and environmental triggers that lead to emotional eating (e.g., stress, boredom, loneliness, anxiety) and implement mindful techniques (breathing, journaling) in order to reduce them.
- Create a structured plan for eating with room for flexibility. Many people who emotionally eat also skip meals, follow restrictive diets, or eat irregularly, which exacerbates cravings and binge behaviors.
- Understand how food affects your mood and energy levels. For instance, blood sugar swings can worsen anxiety and irritability.
Share Link: Can Medical Nutrition Therapy help with emotional eating and stress?
Is Medical Nutrition Therapy covered by insurance?
Several health plans offer MNT benefits, including:
- Aetna
- Blue Cross (note: MNT is billed on the medical side if you have a mental health carve-out)
- Health Alliance Plan
- McLaren
- Medicare Part A (for patients with diabetes and kidney disease)
- Priority Health
Some health plans waive your co-pay and deductible for MNT, while others offer limited or unlimited visits. Although we can speak from our experience on MNT coverage, you are encouraged to contact your health plan and ask the following questions:
- Call the medical side of your health plan vs the behavioral side, as MNT is a medical benefit.
- When calling, ask if you have the benefit for Medical Nutrition Therapy CPT codes 97802 and 97803 and the number of visits you have per calendar year.
- Please note that dietitians must bill under the physician in Michigan, which we do at RCBM, so you will not find the names of the RCBM dietitians listed on your health plan’s roster.
Share Link: Is Medical Nutrition Therapy covered by insurance?
Can I have Medical Nutrition Therapy alongside therapy or medication management at RCBM?
At RCBM, we take an integrative approach to care. All disciplines work together to provide the best experience and outcomes. Most all of the mental health conditions that we treat at RCBM involve a nutrition component, and patients can benefit from medical nutrition therapy, including:
- Addiction
- ADHD
- Anxiety Disorders
- Autism Spectrum Disorder
- Chronic Fatigue and Pain
- Eating Disorders
- Mood Disorders
- Weight Management
Your treatment team works together as we communicate and collaborate on your individual care. In addition, we realize that it is hard to find a dietitian for mental health care in Michigan, so you do not have to be a current patient at RCBM to take advantage of our services.
Share Link: Can I have Medical Nutrition Therapy alongside therapy or medication management at RCBM?
Ready to get started with Medical Nutrition Therapy?
If you are a current patient at RCBM, please contact our office at (248) 608-8800. If you are new to RCBM, you can initiate the admission process by completing a new patient registration form. Once you submit the form, we will match you with one of our registered dietitians. Please note that all appointments are virtual.
We look forward to working with you!
Share Link: Ready to get started with Medical Nutrition Therapy?
Watch: Expert Insights on Medical Nutrition Therapy

Medical Nutrition Therapy
Beverly Price, CEDRD-S, MA discusses the process of Medical Nutrition Therapy (MNT) and how current and prospective patients can access this service to work with our registered dietitians.
Medical Nutrition Therapy at RCBM
In this video what a patient can expect during a typical medical nutrition therapy (MNT) session with a registered dietitian is reviewed. The initial session consists of an assessment to understand eating concerns and overall, health, lifestyle, and nutrition goals. Follow up sessions may include individual meal and grocery planning, macronutrient needs, and realistic support that works for your life.Meet the Providers Who Offer Care for Medical Nutrition Therapy
Beverly Price, RD, MA, CEDS-C, E200-RYT, C-IAYT
Read More
Chelsea Butler, RDN, MSN (formerly Carpentier)
Read More
Jessica Grzybowski, RDN
Read More
Medication Management

At the Rochester Center for Behavioral Medicine, many of our treatment plans incorporate neuropsychiatric medication as part of a comprehensive psychiatric evaluation and approach to mental health care. If you are exploring how to find the right psychiatrist for medication management or wondering whether medication is the right choice for your symptoms, our team provides expert guidance tailored to your needs.
Our Approach
● Diagnostic Screening: Before prescribing medication, we conduct thorough psychiatric assessments to gain a deep understanding of your concerns. This foundational step ensures that our child psychiatrists and other specialists develop treatment plans rooted in accuracy and empathy. If you are searching for a child psychiatrist near me, our team provides expert care designed for younger patients facing emotional and behavioral challenges.
● Collaborative Care: Medication management is most effective when combined with other therapeutic modalities. Our prescribers collaborate closely with therapists and nutritionists to provide holistic mental health care that addresses the mind and body.
Meet Our Specialists
Selecting the right provider for psychiatric medication management is an essential step toward improving mental health. At RCBM, our team of psychiatrists, physician assistants, and nurse practitioners specializes in different treatment areas. You can review each clinician’s biography to find a provider with expertise in your specific condition, whether that includes child psychiatrists for pediatric care or specialists in complex medication regimens.
BrightKaire
At the Rochester Center for Behavioral Medicine (RCBM), we’re excited to adopt BrightKaire, an innovative blood test developed by NeuroKaire that helps match patients with the antidepressant most likely to work for them. By analyzing the biological signature of brain cells and applying advanced AI, BrightKaire aims to reduce the frustrating trial-and-error process often associated with treating depression. Founded in 1993, RCBM remains committed to bringing cutting-edge tools like this to our patients as part of our mission to provide leading, evidence-based mental health care. Learn more by watching Dr. Young's video below:
Spravato Program
Major Depressive Disorder (MDD) is one of the most common mental health disorders in the United States. Treatments such as psychotherapy, medication management, and lifestyle changes may help relieve symptoms. However, other individuals may have Treatment-Resistant Depression (TRD) and continue to experience symptoms such as persistent feelings of sadness, sleep disturbances, low energy, and thoughts of death or suicide despite trying multiple treatments.
SPRAVATO® is the first nasal spray medication specifically for adults with treatment-resistant depression and major depressive disorder with suicidal thoughts or actions. Note: As of February 2025, the FDA has approved Spravato as monotherapy for adults living with treatment-resistant depression (TRD).
Learn more about our Spravato Treatment Resistant Depression Clinic here
Watch: Expert Insights on Medication Management
Spravato Program at RCBM
Dr. Joel Young discusses the use of Spravato for treatment-resistant depression and how to enroll in our Spravato Program at RCBM.
The Spravato Program at RCBM
Hailee Mika, Spravato Program Coordinator, discusses Spravato and how it helps treatment-resistant depression. She also explains how our program works at RCBM, from referral and authorization to the treatment experience. Note: As of February 2025, the FDA has approved Spravato as monotherapy for adults living with treatment-resistant depression (TRD).
How to prepare for a medication check up
Kim Roznwski, PA-C explains how you can best prepare for your medication appointment, including letting your RCBM provider know of any changes in your medication from other providers and how you feel on any new medication or adjustments to current medications. Completing the pre-visit survey prior to your appointment assists your provider in tracking your progress. In addition, having a scale and blood pressure monitor at home is helpful to report information at your virtual medication appointment for proper prescribing. And don't forget to make sure your WiFi is working!
How to Talk to a Loved One About Psychiatric Treatment
Jamie Clark, LMSW explains the best way to discuss mental healthcare with your loved one including finding a safe, comfortable and private place to express how each of you feel. It's imperative to stress the importance of not only physical but mental health care along with assisting your loved one in finding resources.
What Should a Patient Know Before Starting an Antidepressant
Chris Discenna, PA-C sets your expectations for starting antidepressant medication, including not to expect immediate improvement as medications take time to work, side effects you may experience and how to manage, along with the possibility of you needing a dose adjustment or a different antidepressant agent. Combining medication with therapy is highly recommended for a more comprehensive approach for long term outcomes.
BrightKaire with Dr. Young
Joel Young, MD, explains BrightKaire, an innovative, evidence-based tool by NeuroKaire. BrightKaire is a blood test that helps guide antidepressant treatment. By analyzing biological signals in a patient's blood that reflect the activity and health of brain cells, it can predict which antidepressant works best for an individual patient. This brings precision to psychiatric treatment and to decision-making very early on, improving outcomes.Mind Body Program

RCBM believes that mind and body wellness are inextricably linked particularly a personalized and integrative approach to mind and body health. For this reason, it is important to consider how an individual's psychiatric and physical well-being can be addressed to treat the whole person. A major focus on mind and body wellness can be achieved through mindfulness and/or other therapeutic modalities that may also use body-centered therapies such as yoga and meditation.
Mind and body medicine focuses on the connections of the brain to the body and how emotions, verbalizations, behaviors, and spirituality directly affect health and well-being. It is a cognitive and behavioral therapeutic practice that enhances awareness of thoughts and actions to improve self-esteem and self-confidence to live the life desired.
Mind and body medicine uses a multi-disciplinary approach. Several clinical studies indicate integrative therapies can help patients cope and manage pain, minimize stress and anxiety, and gain an overall sense of control over one’s mind and body.
Many of our clinicians believe in the mind-body connection and use this orientation in sessions with their RCBM patients.
Watch: Expert Insights on Mind Body Program

"Mindfulness" A conversation with Dr. Melissa Oleshansky
Dr. Melissa Oleshansky explains the importance of mindfulness and being present in her sessions and how she encourages others to live their best lives.
Women and Trauma
Melissa Oleshansky, PhD discusses how she works with women recovering trauma, including CBT, trauma-focused or gentle-body based therapy. Dr. Oleshansky also recommends daily health habits to reduce stress and walks you through deep breathing and grounding exercises.Meet the Providers Who Offer Care for Mind Body Program
Melissa Oleshansky, PhD, LP, RYT
Read More
Beverly Price, RD, MA, CEDS-C, E200-RYT, C-IAYT
Read More
Chelsea Butler, RDN, MSN (formerly Carpentier)
Read More
David Price, MA, LPC, CAADC
Read More
Jessica Grzybowski, RDN
Read More
Katie Young, MSN, NP, PMHNP-BC
Read More
Related Titles from the RCBM Reading and App list:
Mindfulness: An eight-week plan for finding peace in a frantic world - By Mark Williams & Danny PenmanMindfulness in Everyday Life - By Austin Ortiz
Radical Acceptance: Embracing Your Life with the Heart of a Buddha - By Tara Brach
The Burnout Workbook: Advice and Exercises to Help You Unlock the Stress Cycle - By Smart Recovery
The Mindful Path to Self-Compassion - By Christopher K. Germer, PhD
The Mindful Self-Compassion Workbook: A Proven Way to Accept Yourself, Build Inner Strength, and Thrive - By Kristin Neff and Christopher Germer
Wherever You Go There You Are: Mindfulness Meditation in Everyday Life - By Jon Kabat-Zinn
HabitBull - Simple to use and has so many ways you can collect data
Keep It Green- (iphone) - Data collection and habit “streak” tracker
Sessions- (iphone only) – Activity timer and Data collection/Habit Tracker
10% Happier
Insight Timer - Mindfulness App
Mindfulness Coach
Stop, Breathe, & Think
Wildflowers
Breath2Relax
Atoms. - Atomic Habits Book Companion App
Finch Self-Care App
Mood Disorders

Mood disorders are characterized by symptoms that can significantly affect a person's stability and overall well-being. These mood changes must be severe or repetitive enough to impact daily life.
FAQs
What are the different types of mood disorders?
Mood disorders include:
Depression
Depressive symptoms may include feeling sad or hopeless, as well as difficulties with thinking, memory, eating, and sleeping. A diagnosis of clinical depression requires symptoms to persist for at least two weeks.
There are several different types of depression, including:
Depression with psychosis
Severe depression combined with psychotic episodes is characterized by hallucinations (seeing or hearing things that others don't) or delusions (having fixed but false beliefs). People who experience depression with psychosis have an increased risk of suicidal thoughts.
Dysthymia or Persistent Depressive Disorder (PDD)
Dysthymia is a mild but persistent form of Major Depressive Disorder (MDD). It exhibits the same symptoms as sadness or loss of interest in activities that the individual once enjoyed, changes in sleep patterns, appetite, energy level, concentration, daily behavior, and self-esteem. It is a chronic type of depression, typically milder in severity but lasting for two years or more.
Major Depressive Disorder (MDD)
Individuals with Major Depressive Disorder (MDD) often experience persistent and intense feelings of sadness or a lack of interest in activities they used to enjoy. They may also notice changes in their sleep patterns, appetite, energy levels, concentration, daily behavior, and self-esteem for a period of two weeks or more.
Postpartum depression (peripartum depression)
Postpartum depression is a type of depression that can occur in women and people assigned female at birth (AFAB) during pregnancy or after giving birth. The hormonal, physical, emotional, financial, and social changes that occur after having a baby can lead to symptoms of postpartum depression.
Seasonal affective disorder (SAD)
Seasonal Affective Disorder (SAD) is a type of depression that occurs during specific seasons of the year. It usually starts in late autumn or early winter and lasts until spring or summer. In some cases, SAD episodes might begin in late spring or summer. The symptoms of winter SAD are similar to those of major depression, but they typically improve or diminish during the spring and summer months.
Bipolar disorder
Bipolar disorder is a lifelong mood disorder and mental health condition that causes intense shifts in mood, energy levels, thinking patterns, and behavior. There are several types of bipolar disorder, which involve experiencing significant fluctuations in mood, known as hypomanic/manic and depressive episodes.
There are four basic types of bipolar disorder, including:
Bipolar I disorder
People with bipolar I disorder have experienced one or more episodes of mania. Most people with bipolar I will have episodes of both mania and depression. An episode of depression isn’t necessary for a diagnosis.
Bipolar II disorder
Bipolar II disorder causes cycles of depression similar to those of bipolar I. Individuals with this condition also experience hypomania, which is a less severe form of mania. Hypomanic periods aren’t as intense or disruptive as manic episodes, and those with bipolar II disorder are usually able to handle daily responsibilities.
Cyclothymia disorder (cyclothymia)
People diagnosed with cyclothymic disorder have a consistently unstable mood, experiencing periods of hypomania and mild depression for at least two years.
Other specified and unspecified bipolar and related disorders
Symptoms of this type of bipolar disorder do not meet the criteria for one of the other types, but individuals still experience significant, abnormal mood changes.
Other mood disorders
Other mood disorders include:
Premenstrual dysphoric disorder (PMDD)
This mood disorder typically occurs seven to 10 days before menstruation and resolves within a few days after the start of the menstrual period. It is considered a more severe form of premenstrual syndrome (PMS). Researchers believe hormonal changes associated with the menstrual cycle are responsible for this condition. Symptoms may include anger, irritability, anxiety, depression, and insomnia.
Disruptive mood dysregulation disorder (DMDD)
Disruptive Mood Dysregulation Disorder (DMDD) impacts children and adolescents. It is characterized by frequent anger outbursts and irritability disproportionate to the situation. DMDD is more severe than Intermittent Explosive Disorder (IED), and the anger is present most of the time, typically starting before the age of 10.
Share Link: What are the different types of mood disorders?
What are the causes of mood disorders?
Several factors contribute to the development of mood disorders, including:
Biological: The amygdala and orbitofrontal cortex are the brain areas responsible for controlling feelings and emotions. Studies have shown that people with mood disorders often have an enlarged amygdala on brain imaging tests.
Genetic: Individuals with a strong family history of mood disorders are more likely to develop mood disorders themselves, indicating that genetics plays a role in inheriting mood disorders.
Environmental: Stressful life changes like the loss of a loved one, chronic stress, traumatic events, and childhood abuse are significant risk factors for developing mood disorders later in life, particularly depression. Additionally, depression has been connected to chronic illnesses such as diabetes, Parkinson's disease, and heart disease.
Share Link: What are the causes of mood disorders?
How are mood disorders diagnosed?
RCBM is committed to accurately and thoroughly diagnosing mood disorders in individuals of all ages through our psychological screening process. All patients undergo a comprehensive diagnostic interview to understand their history and current concerns. Additionally, psychological testing helps us pinpoint the specific type of mood disorder along with co-occurring disorders.
Share Link: How are mood disorders diagnosed?
How are mood disorders treated at RCBM?
Psychotherapy
Cognitive behavioral therapy (CBT): This structured and goal-oriented psychotherapy is used by mental health professionals to treat or manage mental health conditions and emotional concerns. CBT combines behavioral exposure therapy and cognitive restructuring to help the patient confront avoidance, correct negative automatic thoughts, and return to optimal functioning.
Dialectical behavior therapy (DBT): DBT is a form of talk therapy based on cognitive behavioral therapy (CBT) but specifically adapted for individuals with intense emotions.
Psychodynamic therapy: This type of therapy is based on the concept that behavior and mental well-being are influenced by experiences during childhood and problematic repetitive thoughts or feelings that are outside of your awareness.
Medication management
Medications that RCBM providers may prescribe to help treat mood disorders include:
Antidepressants: The most commonly used drugs to treat depression and depressive episodes of bipolar disorder are selective serotonin reuptake inhibitors (SSRIs). Similar to SSRIs in their action, serotonin and norepinephrine reuptake inhibitors (SNRIs) are also frequently prescribed. Although studies indicate that different types of antidepressants work equally well, some may be more effective for certain individuals. Typically, it takes four to six weeks for an antidepressant to begin working. It is crucial to take antidepressants as prescribed and continue taking them even if you start feeling better.
Mood stabilizers: Certain medications are used to regulate mood swings associated with conditions like bipolar disorder. These medications work by reducing abnormal brain activity. In some cases, healthcare providers may prescribe mood stabilizers alongside antidepressants. Some commonly used mood stabilizers include lithium and anticonvulsant drugs.
Antipsychotics (neuroleptics): People experiencing mania or mixed episodes in bipolar disorder may be treated with atypical antipsychotic drugs. Atypical antipsychotics are also prescribed to treat depression if symptoms aren’t controlled with an antidepressant alone..
SPRAVATO®
RCBM has a robust SPRAVATO® program. SPRAVATO® (esketamine), is manufactured by Janssen Pharmaceuticals. This medication is used adjunctively with antidepressant medications for treatment-resistant depression. Our medical director, Dr. Joel Young, was a primary investigator during the SPRAVATO® clinical trial.
Taken along with an oral antidepressant, SPRAVATO® is the first nasal spray medication specifically for adults with treatment-resistant depression.
Taken along with an oral antidepressant, SPRAVATO® is the first nasal spray medication that treats depressive symptoms in adults with major depressive disorder with suicidal thoughts or actions.
Medical Nutrition Therapy
Balanced nutrition can play a vital role in managing depression symptoms and supporting mental health. Our registered dietitians can develop a personalized nutrition plan to help with the management of depression.
Share Link: How are mood disorders treated at RCBM?
Can you tell me more about RCBM’s Spravato program?
Major Depressive Disorder (MDD) is one of the most common mental health disorders in the United States. Treatments such as psychotherapy, medication management, and lifestyle changes may help relieve symptoms. However, other individuals may have Treatment Depression (TRD) and continue to experience symptoms such as persistent feelings of sadness, sleep disturbances, low energy, and thoughts of death or suicide despite trying multiple treatments.
Taken along with an oral antidepressant, SPRAVATO® is the first nasal spray medication specifically for adults with treatment-resistant depression.
Taken along with an oral antidepressant, SPRAVATO® is the first nasal spray medication that treats depressive symptoms in adults with major depressive disorder with suicidal thoughts or actions.
The U.S. Food & Drug Administration approved SPRAVATO® on March 5, 2019, and is only available to patients at certified treatment centers in the United States, such as Rochester Center for Behavioral Medicine (RCBM).
SPRAVATO® is a prescription medication, used along with an antidepressant taken by mouth, for TRD in adults.
This treatment is approved for adults ages 18 and older.
Learn more about our SPRAVATO® program here.
Share Link: Can you tell me more about RCBM’s Spravato program?
How effective is treatment for mood disorders at RCBM?
Psychotherapy
CBT is particularly effective for mood disorders. The hallmark of CBT is the patient’s role in learning and practicing skills outside the session to maximize the therapeutic benefit of this therapy. In mood disorders, the patient will learn coping skills to master tasks often thought too arduous for the depressed patient. The use of CBT with or without medication management is addressed, and the ultimate decision is made between the patient and the RCBM Professional.
Medication Management
The process of finding the right medication to treat your specific mood disorder might involve some trial and error. Your healthcare provider could initially prescribe a specific drug taking into consideration any other issues you may be dealing with, like anxiety or difficulty sleeping, or based on their prior success in treating depression in other patients.
Please remember that it may take up to eight to 12 weeks of consistently taking antidepressants as prescribed to see their full benefit and to determine whether a medication is a good fit for you or if another option may be better.
Medical Nutrition Therapy
Studies show that regular meals help maintain blood sugar levels and support overall mood stability. In addition, foods high in omega-3 fatty acids, such as fish, nuts, and seeds, fight free radicals and oxidative stress that cause depression symptoms.
Fruits and vegetables contain polyphenols, a significant compound in managing depression symptoms and supporting mental well-being.
Spravato Program
In clinical studies, patients who achieved stable remission with SPRAVATO® augmented with an antidepressant showed a 51% decrease in risk of relapse. In addition, there was a 70% risk reduction for depressive symptoms among those who achieved a stable response compared to an antidepressant alone.
For individuals with TRD
In clinical studies, improvement of depressive symptoms was demonstrated at four weeks by SPRAVATO® plus an oral antidepressant, compared with a placebo nasal spray plus an oral antidepressant. Not all patients will respond to SPRAVATO®.
For individuals with MDSI
In clinical studies, those who took SPRAVATO® and an oral antidepressant experienced a more significant reduction of depressive symptoms at 24 hours compared to those who took a placebo plus an oral antidepressant. Further decreases were seen consistently through four weeks (25 days) of treatment, so following your healthcare provider's treatment plan is essential. Not all patients will respond to SPRAVATO®.
Share Link: How effective is treatment for mood disorders at RCBM?
How do I get started with treatment for mood disorders at RCBM?
If you are a current patient at RCBM, don't hesitate to contact our office at (248) 608-8800. If you are new to RCBM, you can initiate the admission process by completing a new patient registration form. Once you submit the form, we will match you with one of our qualified clinicians who specializes in treating mood disorders. Please note that individuals must be residents of Michigan. We are committed to helping you, or your loved one live a quality life and look forward to working with you.
How do I get started with treatment in our SPRAVATO® program?
All patients, including external patients referred by their healthcare provider, are required to be evaluated by an RCBM medical provider prior to referral to the SPRAVATO® program. If you are a current patient interested in our program, please schedule an appointment with your provider to determine if the program is an appropriate fit for you.
Patients must have an active diagnosis of either Treatment Resistant Depression (TRD) or Major Depression with Acute Suicidal Ideation (MDSI) to be eligible for treatment with SPRAVATO®.
Patients must have tried and failed several anti-depressant medications along with augmentations. Other exclusions are found on the SPRAVATO® page of our website, along with information on insurances that cover SPRAVATO® treatment.
Share Link: How do I get started with treatment for mood disorders at RCBM?
Watch: Expert Insights on Mood Disorders

What is Major Depressive Disorder?
David Price, LPC, CAADC expounds on major depressive disorder (MDD) along with coping mechanisms for individuals with MDD.
What is Seasonal Affective Disorder?
Karolina Redziniak, LLP explains seasonal affective disorder (SAD), a type of depression that affects people in the fall and winter months, along with the signs, symptoms and treatment.
What is Dialectical Behavioral Therapy?
Aundreah Walenski, LMSW discusses the components of dialectical behavioral therapy (DBT), an evidence-based psychotherapy that is used to treat personality disorders and interpersonal conflicts and how this modality can help individuals live the life they want to live.
What is Cognitive Behavioral Therapy (CBT)?
Dr. Melissa Oleshansky, PhD discusses cognitive behavioral therapy (CBT). This structured and goal-oriented psychotherapy is used at RCBM to treat or manage mental health conditions, stress, unhealthy habits, and emotional concerns.
What is Bipolar Disorder?
Jennifer Lindsey, LMSW explains the differences between bipolar 1, bipolar 2, and cyclothymia along with describing their mood states.
What is the treatment for bipolar disorder?
Jennifer Lindsey, LMSW explains the treatment for bipolar disorder that includes medication management, CBT, DBT, sleep hygiene, rhythmic exercise, support groups, and family education.
The Spravato Program Referral Process
Hailee Mika, Spravato Program Coordinator, explains how Spravato works for treatment-resistant depression and how to refer patients to the Spravato Program at RCBM. Note: As of February 2025, the FDA has approved Spravato as monotherapy for adults living with treatment-resistant depression (TRD).
The Spravato Program Treatment Experience at RCBM
Hailee Mika, Spravato Program Coordinator, discusses your experience in our Spravato Program and eligibility requirements.
Spravato Program at RCBM
Dr. Joel Young discusses the use of Spravato for treatment-resistant depression and how to enroll in our Spravato Program at RCBM.
What is Borderline Personality Disorder (BPD)?
Riley Ubben, LMSW explains borderline personality (BPD). Those who struggle with BPD experience intense emotions, are impulsive in their actions, have a strong fear of abandonment and a distorted self-image. Psychotherapy can help individuals with BPD improve their symptoms.
What is Premenstrual Dysphoric Disorder (PMDD)?
Elizabeth Sweet, PMHNP-BC, MSN discusses PMDD, which is a severe form of premenstrual syndrome (PMS) that causes intense emotional and physical symptoms, such as extreme mood swings, anxiety, and depression, in the week or two before menstruation. These symptoms can significantly disrupt daily life and relationships. Lizz also discusses treatment options.
When Mental Health Symptoms Warrant Urgent Care - But Not the ER
Jennifer Stone, LPC, NCC, CAADC discusses when to go to the emergency room for treatment vs urgent care. If you are an immediate risk to yourself including self-harm behaviors or suicidal thoughts, and/or the thought of doing harm to others, an ER visit is warranted. An urgent care visit would be warranted for non life threatening symptoms that impact daily living such as depression, anxiety, panic attack or sleep disturbances. In this situation, stabilization can take place with referral to a professional, such as RCBM clinicians, for long term management.
College Mental Health
Melissa Oleshansky, PhD, RYT, gives advice on how to protect your mental health at college. She cautions against confusing overachievement with wellbeing, as saying yes to everything can leave you depleted. Know when to slow down, create space to think and feel, build in daily movement and fresh air, or call someone. Reach out early - asking for help from a therapist, friend, or family is not a weakness, it's emotional intelligence. You are worth taking care of.Related Titles from the RCBM Reading and App list:
Depression Fallout: The Impact of Depression on Couples & What you can do to preserve the bond - By Anne SheffieldHow you can survive when they’re depressed - By Anne Sheffield
Overcoming Bipolar Disorder: A Comprehensive Workbook for Managing Your Symptoms and Achieving Your Life Goals - By Mark Bauer, Amy Kilbourne, Devra Greenwald, Evette Ludman, and Linda McBride
Rock Steady: Brilliant Advice from My Bipolar Life - By Ellen Forney
What to do when someone you love is depressed - By Mitch Golant & Susan Golant
DBT Coach - DBT Skills and Mood Tracking
Daylio - Daily Mood Tracking App
BeyondNow App
Calm Harm - Self-Harm App
Obsessive-Compulsive Disorder

Obsessive-compulsive disorder (OCD) is a mental health disorder characterized by obsessions (repetitive, frequent, unwanted/disturbing thoughts, images, or impulses) and compulsions (mental or physical acts that a person intentionally performs to reduce the distress caused by the obsessions). OCD can occur across the lifespan, starting in early childhood (e.g., preschool) for some, adolescence for others, and adulthood for others.
Individuals with OCD describe “having/needing” to do a compulsion because of the fear/anxiety associated with the obsession. They do not want to do this, but feel that this is the only option when faced with an obsession. This leads to a very vicious cycle and can cause considerable disruption in areas of functioning and further distress for the individual with OCD.
How is OCD Treated?
At RCBM, we treat OCD using the gold-standard approach of exposure and response prevention (ERP). ERP involves safely and methodically exposing an individual to a feared situation and committing to not engage in compulsive behavior. Over time, ERP retrains the person with OCD’s brain to no longer see the obsession as something to be fearful of, as well as reducing the time-consuming compulsions. The individual with OCD and their therapist will create an exposure plan that feels tolerable to the patient. There are times when treating OCD with ERP is not enough – research has demonstrated that the most effective approach is often a combination of ERP and medication. You will work with your therapist to decide if this is the best treatment option for you.
Transcranial Magnetic Stimulation (TMS)
In addition, Repetitive Transcranial Magnetic Stimulation (rTMS) is an innovative, FDA-cleared treatment that offers new hope for adults living with OCD, who haven’t found relief with medication alone. rTMS is a non-invasive therapy that targets the root of OCD without surgery, sedation, or downtime.
At RCBM, we use NeuroStar® Advanced Therapy, which is the #1 physician-recommended rTMS treatment. OCD treated with rTMS has been shown to improve symptoms. A total of 57.9% of patients showed a greater than 30% reduction in the severity of OCD symptoms, and 52.4% experienced a sustained response.
Learn more about RCBM's rTMS program here
Meet the Providers Who Offer Care for Obsessive-Compulsive Disorder
Alexandra Siegel, MA, LLP
Read More
Aundreah Walenski, LMSW
Read More

Mindy Layne Young, MSW, CSW, JD
Read More
Older Adults
The aging population has its own set of special needs. As individuals age, they face difficult issues such as loss of mobility and independence, the loss of loved ones, and sometimes memory loss. The geriatric treatment clinicians at RCBM are sensitive and understanding when it comes to helping you, or your aging loved ones, cope with this often challenging but wonderful time in their lives.
We assist the geriatric population with many different services. Not only do we help with medication management, but we also provide individual psychotherapy.
Opiate Addiction

Non-medical use of opiates is dramatically increasing the United States (U.S.). Opiates include prescription drugs such as Vicodin and Oxycontin, as well as street drugs such as heroin. The misuse of and addiction to opioids—including prescription, pain relievers, heroin and synthetic opioids such as fentanyl—is a serious national crisis. Abuse of and dependence on opiates interfere significantly with work, relationships, and education.
At RCBM, we offer a collaborative approach to treating opiate-related struggles. Individuals with opiate addiction or dependence are evaluated and treated for other psychiatric problems which may be contributing to their opiate use. Suboxone is a medication used to aid in the cessation of opiate use while controlling withdrawal symptoms. Suboxone may be prescribed as a part of the treatment plan. Individuals on Suboxone are required to take part in counseling. Outside resources such as Narcotics Anonymous are also provided for additional support.
Watch: Expert Insights on Opiate Addiction
Addiction and Relapse Prevention During COVID-19
Whenever there's a time of high stress, the risk of relapse or the risk of escalating use is increased. Judy Redmond, MA, LPC, LLP, CAADC and Aliya Pasik, PA-C discuss relapse prevention during COVID-19.
Addiction Treatment
Aliya Pasik, PA-C, Program Director, Addiction Recovery Clinic discusses the RCBM Addiction Medicine Program at RCBM.
Addiction, Signs and Recovery | with Aliya Pasik, MS, PA-C
Aliya Pasik, MS, PA-C, is the Program Director of the Addiction Recovery Center at the Rochester Center for Behavioral Medicine. Aliya addresses the many forms of addiction and substance abuse, particularly as it relates to the 50+ demographic. She describes underlying conditions that lead to self-medication such as ADHD, loneliness, anxiety, depression, and boredom. Alcohol abuse seems to be on the rise, especially during the Coronavirus pandemic. Aliya also discusses specific clinical programs that she is spearheading, describes certain signs that lead to substance abuse, and provides medical, cognitive, and holistic ways for patients and their families to have conversations that lead to recovery.Overview of RCBM Services
The Rochester Center for Behavioral Medicine offers an array of mental health and substance abuse services in our comprehensive outpatient setting. Our practitioners work collaboratively within their expertise, through medication management, psychotherapy, and nutrition therapy, in order to deliver the highest quality care.
Parenting Techniques

It is not uncommon for RCBM clinicians to be faced with overwhelmed parents, many of whom have attempted to implement a variety of parenting techniques but have not found success. These failed attempts can lead to feelings of hopelessness and helplessness for these parents, which often exacerbate the problematic dynamics in the household.
The key elements include consistency and remaining calm, both of which can be difficult during stressful parenting situations. Our therapists at RCBM take into consideration the age of the child, the presenting concerns, and the family dynamics in order to tailor a treatment plan. Often, therapists will use a combination of techniques to meet their needs. These may include education about special considerations for their child along with exploration and practicing of parenting techniques. Sessions with the child alone, the caregivers alone, and the family together are all integral parts of the treatment plan.
Watch: Expert Insights on Parenting Techniques

Harmony at Home
RCBM staff shares ways to promote positive family and spousal interaction during COVID-19.
Screen Time During COVID-19
RCBM's Aundreah Walenski, LMSW discusses appropriate screen time for children in an interview with Taryn Asher, Fox 2 TV.
Make this Summer Successful for Your Children
With COVID-19 in our midst, it will be an unusual summer for many families. RCBM's Kathy Pritchard spoke to FOX 2 Detroit about how to make it a successful summer...structure is the key.
How to prepare your child or teen for therapy
Kathy Huyghe, LMSW discusses when is the right time for your children to get help through psychotherapy. She explains the circumstances where therapy can help children and teens and gives suggestions on how to talk to them about what to expect in therapy.
Screen Time for Kids and Teens
Elizabeth Sweet, PMHNP-BC, MSN discusses the impact of screen time on mental health along with guidance for parents such as checking your child's viewing history, making sure that apps downloaded are age appropriate and being attuned to unregulated apps. Other helpful suggestions are also given including paying attention to your child's behavior based on what they are viewing and having scheduled screen time.
ADHD Medication Isn’t Enough - What Else Can Help Your Child Focus?
Ashley Crowder, MA, LPC, discusses how to help your child stay focused when their ADHD medication does not last all day. This includes a schedule with routine along with unstructured time for creativity. Visual schedules including chore charts that can be checked off upon completion along with reward stickers that can lead to non-monetary awards.Related Titles from the RCBM Reading and App list:
123Magic - By Thomas Phelan, PhDBoys Adrift: The Five Factors Driving the Growing Epidemic of Unmotivated Boys and Underachieving Young Men - By Leonard Sax
Good Inside - By Dr. Becky Kennedy
I Love My Kids, But I Don’t Always Like Them: Expert Advice for Parents of Challenging Children - By Franki Bagdade
Mindful Parenting - By Kristen Race
No Drama Discipline - By Dr. Daniel Siegel
Parenting from the Inside Out - By Daniel Siegel and Mary Hartzell
Parenting Teen Boys: An Effective Guide for Raising Teen Boys - By Elizabeth Roxas
Survival Tips for Parents of Teen Boys - By Mitch DeArmon
The New Strong-Willed Child - By James Dobson, PhD
ClearLock
OurPact
School Advocacy

The Rochester Center for Behavioral Medicine works with children, parents, and schools to provide a comprehensive and integrated treatment program. Children and teenagers spend the majority of their day in the school setting, and their relationships and behaviors in the school setting are often critical pieces of the diagnostic and treatment puzzle. Your child’s therapist or doctor will contact the school to ensure that treatment plans and goals are aligned and well-coordinated.
Navigating the educational system to advocate for your child can be overwhelming. RCBM can assist your family in getting answers to the follow types of questions: How do I know if my child is eligible for an Individualized Education Plan (IEP) or a 504 Plan for my child? When and how do I suggest this to my child’s school? What type of accommodations will teachers make without an official plan? Clinicians at the Rochester Center for Behavioral Medicine are well-versed in these issues and can help your family work through this process.
Watch: Expert Insights on School Advocacy

School Accomodations
Lizzy Thompson, NP discusses accommodations parents can ask for in the school setting including a 504 plan or individualized education program (IEP) that help protect students with learning differences to access the full potential of academic support. Lizzy also conveys recommendations as to how parents should work with schools setting the stage in which schools have to reply and make recommendations.Sexual Health and LGBTQ Services
Many people struggle with questions and feelings surrounding their sexuality, intimate relationships, sexual orientation, sexual trauma, sexual behaviors, and gender identity. This can be very isolating, confusing, and frustrating. Often people are uncomfortable seeking assistance or discussing these topics with mental health professionals due to fear of negative responses or biased attitudes from staff or other clientele. Additionally, the lesbian, gay, bisexual, transgender, queer, and questioning (LGBTQ) community can experience higher negative mental health outcomes due to community prejudice/biases and are almost three times more likely than others to experience a mental health condition such as major depression or generalized anxiety disorder.
The Rochester Center for Behavioral Medicine believes that sexual health and identity are vital to overall mental well-
 being. We strive to provide caring, affirming, and confidential services in an all-inclusive space that is supportive and free from bias. We have a dedicated multidisciplinary staff that is skilled in providing sexual health and LGBTQ services to individuals, couples, and families of all backgrounds and ages.
being. We strive to provide caring, affirming, and confidential services in an all-inclusive space that is supportive and free from bias. We have a dedicated multidisciplinary staff that is skilled in providing sexual health and LGBTQ services to individuals, couples, and families of all backgrounds and ages.
Related Titles from the RCBM Reading and App list:
Always my Child - By Kevin JenningsBeyond Acceptance: Parents of Lesbians & Gays Talk About Their Experiences - By Carolyn W. Griffin & Marian J. Wirth
Is it a Choice? - By Eric Marcus
Love Ellen: A Mother/Daughter Journey - By Betty Degeneres
My Child is Gay: How Parents React When They Hear the News - By Bryce McDougall
Out of the Ordinary: Essays on Growing up with Gay, Lesbian or Transgender Parents - By Noell Howey & Ellen Samuels
Permanent Partners - By Betty Berzon, PhD
Someone I Love is Gay: How Family & Friends Can Respond - By Anita Worthen & Bob Davies
Straight Parents, Gay Children. Keeping Families Together - By Robert A. Bernstein
Come As You Are: The Surprising New Science That Will Transform Your Sex Life - By Emily Nagoski, PhD
Sexual Health and Wellness

The Rochester Center for Behavioral Medicine believes that sexual health is vital to overall mental well-being. We strive to provide caring, affirming, and confidential services in an all-inclusive space that is supportive and free from bias. We have a dedicated multidisciplinary staff that is skilled in providing sexual health services to adult individuals and couples striving for a healthier and happier relationship with sex and sexuality.
What Areas of Sexual Health Do We Support?
- Absent or low sexual desire or arousal
- Compulsive or excessive sexual behaviors
- Difficulty achieving orgasm
- Difficulties with erection or ejaculation
- Genital and pelvic pain with sexual activity
- Intimate Relationship Issues
- Substance or medication-induced sexual dysfunctions
- Perinatal, postpartum, or perimenopausal sexual changes
- Sexual dysfunction related to sexual trauma
Our Approach to Attaining Sexual Health
- Non-judgmental, thorough, and thoughtful assessment and evaluation of your symptoms
- Individual sexual health counseling
- Couples and marital counseling
- Medication management and evaluation
- Treatment of co-occurring mental health conditions
- Collaborative and coordination of care with your RCBM team and external providers
What You Can Expect
- An initial sexual health assessment with a licensed therapist or medical provider
- Individualized and collaborative treatment planning and recommendations
- Referral to outpatient counseling and medication management if indicated
- Coordination of care with external health providers, if applicable
Sexual Health Program Patient Interest Form:
For patients who have been seen by an RCBM provider within the past 6 months, please DO NOT complete the form below. Please discuss your interest with your RCBM provider at your next appointment. Thank you!
If you are a New Patient to RCBM, please visit the “New Patient” link on the navigation bar at the top of this page and complete registration. You will select on the registration form that you have interest in the Sexual Health Program, and the site will automatically route you to complete the Sexual Health Program Interest Form.
FAQs
Why choose RCBM for sexual health support?
Here at RCBM, we are uniquely suited to treat complex conditions and provide individual treatment plans. When it comes to sexual health, many contributing factors can make our sexual health go awry. Our physical health, mental health, traumatic experiences, and life adjustments ALL can affect our sexual wellness. We offer interdisciplinary services that address your sexual health and much beyond that. We offer individual and couples counseling, medication management, comprehensive testing, medical nutrition therapy, trauma therapy, weight management, and much more that aim to treat your sexual health and the underlying factors that may be the cause of your concerns.
Share Link: Why choose RCBM for sexual health support?
What If I am nervous about discussing intimacy?
Sex is a taboo subject for many. It is natural to be nervous about discussing your intimate life with a healthcare provider. All RCBM sexual health providers take a non-judgmental approach to their treatment and prioritize confidentiality. Additionally, we offer secure telehealth services that enable you to receive care in the comfort and privacy of your own home.
Share Link: What If I am nervous about discussing intimacy?
Can couples attend sessions together?
Absolutely! You can seek out sexual health services individually or as a couple. We see all couples, including those in LGBTQIA+ relationships and consensual non-monogamous relationships. If you are unsure if you should involve your partner or go individually for care, please speak with your sexual health care provider.
Share Link: Can couples attend sessions together?
Watch: Expert Insights on Sexual Health and Wellness

Sexual Intimacy
Aundreah Walenski, LMSW discusses her experience in working with common challenges couples face with sexual intimacy including differing expectations, life events, illness, or trauma. Therapy provides an opportunity to address ways to improve sexual health including communication, education, and other therapies to treat sexual intimacy concerns.
Gender Identity Care
Mckenzie Lopez, LMSW explains who we create a safe space for exploring gender identity at RCBM, including making individuals feel respected and safe to share who they are. We address gender identity concerns in a non-judgmental way to improve overall quality of life. Modalities include cognitive behavioral therapy for anxiety, depression and stress reduction along with trauma informed therapy.Meet the Providers Who Offer Care for Sexual Health and Wellness
Aundreah Walenski, LMSW
Read More
Jennifer Lindsey, LMSW
Read More
Marni Stone, LMSW
Read More

Megan Mio, BSMS, PA-C
Read More
Related Titles from the RCBM Reading and App list:
10 Smart Things Gay Men Can Do To Find Real Love - By Joe Kort, PhD, LMSW10 Smart Things Gay Men Can Do To Improve Their Lives - By Joe Kort, PhD, LMSW
Better Sex Through Mindfulness: How Women Can Cultivate Desire - By Lori A. Brotto, PhD
Come As You Are: The Surprising New Science That Will Transform Your Sex Life - By Emily Nagoski, PhD
Come Together: The Science (and Art!) of Creating Lasting Sexual Connections - By Emily Nagoski PhD
Cracking the Erotic Code, Helping Gay Men Understand Their Sexual Fantasies - By Joe Kort, PhD, LMSW
Erotic Orientation - By Joe Kort, PhD, LMSW
Is My Husband Gay, Straight or Bi? - By Joe Kort, PhD, LMSW
LGBTQ Clients in Therapy, Clinical Issues and Treatment Strategies - By Joe Kort, PhD, LMSW
Mating in Captivity: Unlocking Erotic Intelligence - By Ester Perel
She Comes First: The Thinking Man’s Guide to Pleasuring a Woman - By Ian Kerner, PhD
Side Guys - By Joe Kort, PhD, LMSW
The Better Sex Through Mindfulness Workbook: A Guide to Cultivating Desire - By Lori A Brotto, PhD
Understanding the Sexual Betrayal of Boys and Men, The Trauma of Sexual Abuse - By Joe Kort, PhD, LMSW
Sleep Disorders
Over 50% of adults report difficulty sleeping, half of which suffer with chronic sleep difficulty. We now know that medications are not the only solution to insomnia and that it is possible to successfully treat insomnia using cognitive-behavioral therapy (CBT). CBT has been endorsed by the National Institutes of Health as an effective method for treating insomnia. Research on CBT shows the following:
* 75% of insomnia patients experience significantly improved sleep
* The majority become normal sleepers
* 85- 90% reduce or eliminate sleeping pills
CBT achieves these results because it is based on the idea that insomnia is treated effectively by addressing the underlying causes of insomnia-related thoughts and behaviors, which are learned and can be unlearned.
CBT COMPONENTS
Techniques taught in CBT include:
* changing sleep thoughts and behaviors
* lifestyle habits that improve sleep
* relaxation techniques
WHO WOULD BENEFIT
* individuals with problems falling asleep or waking during the night
* individuals who wish to reduce or eliminate sleep medications
VISITS
CBT for insomnia includes:
* an initial individual assessment
* five individual treatment sessions over a six week period
INSURANCE COVERAGE
CBT is covered by most insurance companies but coverage cannot be guaranteed.
LINK
Studies have shown over 75% of adults with ADHD have difficulty with sleep. Tuck Sleep has created a guide to help combat this issue. Their guide includes a comprehensive overview of ADHD, how it affects sleep, expert sleep management information for people with ADHD and much more.
Watch: Expert Insights on Sleep Disorders

Emma Faruolo - Cognitive Behavior Therapy - Insomnia
Emma Faruolo, MA, explains the CBT-i process in place at Rochester Center for Behavioral Medicine.Sleep Disorders

Over 50% of adults report difficulty sleeping, half of whom suffer from chronic sleep difficulties. We now know that medications are not the only solution to insomnia and that cognitive-behavioral therapy (CBT) can be successfully used to treat it. The National Institutes of Health has endorsed CBT as an effective method for treating insomnia. RCBM uses a program called CBT-I for the treatment of sleep disorders.
FAQs
How is CBT-I used to treat sleep disorders at RCBM?
CBT-I Components Techniques taught in CBT-I include:
- Changing sleep thoughts and behaviors
- Lifestyle habits that improve sleep
- Relaxation techniques
Components of CBT for insomnia include:
Five individual treatment sessions over six weeks (Sessions 1-3 once per week, skip a week, session 4, skip a week, session 5)
Share Link: How is CBT-I used to treat sleep disorders at RCBM?
Who would benefit from CBT-I?
- Individuals with problems falling asleep, waking during the night, or waking too early
- Individuals who wish to avoid, reduce, or eliminate sleep medications
- Individuals who are truly motivated to sleep better and can engage in self-management, including keeping appointments, completing a sleep diary, maintaining a consistent arising time, and reducing time in bed.
Share Link: Who would benefit from CBT-I?
What are the patient responsibilities for participating in the CBT-I program?
- Weekly reading in a book participant purchases called “Say Goodnight to Insomnia.”
- Weekly reading of the session summary handout that accompanies the book
- Daily writing of sleep information in the “sleep diary” log
- Daily writing of negative and positive sleep thoughts on the provided "thought log."
- Practicing guided relaxation using MP3 audio provided via email
- Practicing sleep modification behaviors and other habit changes as guided by the program
Share Link: What are the patient responsibilities for participating in the CBT-I program?
How effective is CBT-I for sleep disorders?
Research on CBT-I shows the following:
- 75% of insomnia patients experience significantly improved sleep
- The majority become normal sleepers
- 85- 90% reduce or eliminate sleeping pills
- CBT achieves these results because it is based on the idea that insomnia is treated effectively by addressing the underlying causes of insomnia-related thoughts and behaviors, which are learned and can be unlearned
Share Link: How effective is CBT-I for sleep disorders?
How do I get started with CBT-I treatment at RCBM?
If you are a current patient at RCBM, don't hesitate to contact our office at (248) 608-8800. If you are new to RCBM, you can initiate the admission process by completing a new patient registration form. Once you submit the form, we will match you with one of our qualified clinicians specializing in CBT-I treatment for sleep disorders. Please note that individuals must be residents of Michigan and willing to visit the office if necessary. If we participate with your insurance, CBT-I is billed as psychotherapy visits. We are committed to helping you get the treatment you need and look forward to working with you.
Share Link: How do I get started with CBT-I treatment at RCBM?
Watch: Expert Insights on Sleep Disorders
What is CBT-I?
Julia Rodgers, BSN, LLMSW explains RCBM's CBT-I program - a - 6 week treatment program that focuses on identifying, along with changing thinking, feeling and behaving that contributes to sleep challenges. CBT-I is the gold standard of care for insomnia.
CBT-I and Chronic Insomnia
Julia Rodgers, BSN, LMSW heads the cognitive behavioral therapy program for insomnia. She presents approaches used at RCBM including targeting unhelpful sleep thoughts and behaviors, and addressing the root cause of insomnia through CBT-I by exploring fears. while shifting thinking and behavior.Related Titles from the RCBM Reading and App list:
Quiet Your Mind and Get to Sleep: Solutions to Insomnia for those with Depression, Anxiety, or Chronic Pain - By Colleen Carney and Rachel ManberCBT-i Coach - Sleep Disorders App
Social Phobia

Social Phobia, also known as Social Anxiety Disorder, is characterized by marked and persistent fear of situations in which one must perform or interact socially with or in front of others. A person with social phobia fears situations where they are exposed to new situations or people. They, therefore, worry about behaving in a way that they might be judged by others as foolish, unacceptable, inappropriate, or inadequate.
When a socially phobic individual is exposed to these situations, they feel anxious, both physiologically and emotionally. This disorder causes a negative impact on the individual’s social, academic and/or occupational functioning. Treatment for social phobia focuses on helping the patient to explore and identify possible triggers to their social anxiety, how this anxiety manifests itself, and develop coping skills and tools to help overcome their phobias. Furthermore, treatment interventions for social phobia may include individual, family, and group therapy. Cognitive-behavioral therapeutic techniques are often utilized, along with relaxation techniques and psychotropic treatment if appropriate.
Spravato® Treatment Resistant Depression Clinic

Have other depression treatments failed? Start your journey to relief with SPRAVATO®
Major Depressive Disorder (MDD) is one of the most common mental health disorders in the United States. Treatments such as psychotherapy, medication management, and lifestyle changes may help relieve symptoms. However, other individuals may have Treatment Depression (TRD) and continue to experience symptoms such as persistent feelings of sadness, sleep disturbances, low energy, and thoughts of death or suicide despite trying multiple treatments.
Explore new hope with treatment resistant depression options at our state-of-the-art SPRAVATO treatment program:
SPRAVATO® (esketamine nasal spray) is a new depression medication and an innovative nasal spray treatment for depression that hasn’t improved with other medications. At the Rochester Center for Behavioral Medicine, we provide safe, in-office SPRAVATO® care with the support of an experienced team.
Our medical director, Dr. Joel Young, was a primary investigator during the SPRAVATO® clinical trial. RCBM has 30+ years of experience helping patients find relief from depression, anxiety, and more, guided by Dr. Joel Young and our trusted clinical team.
Should I choose SPRAVATO® or TMS?
What is SPRAVATO®?
SPRAVATO® is the brand name of esketamine. Esketamine is made from a drug called ketamine, an anesthetic that has also been used for many years to treat depression. Because esketamine is more potent, it can be used at a lower dose and has fewer side effects. SPRAVATO® is a unique treatment for individuals who have treatment resistant depression. It involves the antidepressant esketamine delivered in a nasal spray not responded to oral medications.
While SPRAVATO® and ketamine are chemically related, SPRAVATO® is not the same as ketamine. Only SPRAVATO® has undergone extensive controlled clinical trials that informed the FDA approval of the medicine for use in adults with TRD and to treat depressive symptoms in adults with MDD with acute suicidal ideation or behavior.
How It Works
SPRAVATO® (esketamine) belongs to a class of medications called N-methyl-D-aspartate (NMDA) receptor antagonists. It works differently than conventional antidepressants, which alter concentrations of various neurotransmitters, including dopamine, serotonin, and norepinephrine. By targeting NMDA receptors in the brain, SPRAVATO® boosts glutamate levels, the brain’s most prevalent chemical messenger. By increasing glutamate activity, SPRAVATO® enhances communication between brain cells, helping to stabilize mood and improve cognitive function. This results in a greater reach and more substantial impact on brain cells with a single dose compared to conventional antidepressants, potentially leading to faster and more effective relief of depressive symptoms.
Benefits and Safety
Effectiveness in Treatment Resistant Depression
SPRAVATO® has been specifically effective for individuals with treatment resistant depression. Studies have shown that a significant percentage of these patients experience significant improvement after just a few sessions, offering hope to those who have struggled with finding effective treatments for depression.
Reduction in Suicidal Thoughts
Another vital benefit of SPRAVATO® is its impact on reducing suicidal ideation. Research indicates that SPRAVATO® can quickly decrease the severity of suicidal thoughts. It provides urgent support for individuals in acute distress and potentially prevents tragic outcomes.
Convenience of Administration
SPRAVATO® is administered as a nasal spray, which many patients find more convenient and less invasive than other forms of treatment. The administration process is straightforward and can be done quickly under the supervision of a healthcare provider, making it a practical option for many.
What to Expect
Treatment sessions are conducted in-office and last 2 hours. A medical provider and technician will monitor you throughout the session, and your vitals will be taken at regular intervals.
There are 2 phases of treatment: Induction and Maintenance.
- Induction indicates the start of your SPRAVATO® treatment, which is as follows: 4 weeks of twice-weekly treatment with at least 1 day in between treatment sessions.
- Maintenance indicates your continued SPRAVATO® treatment and is as follows: once weekly treatment weeks 5 - 8; weeks.
- You and your prescriber determine a 9+ weeks treatment schedule and can be once weekly, once every other week, once every 3 weeks, or an alternative schedule.
The duration of your visit will take place in a private treatment room equipped with a recliner, a guest seating area, and amenities such as a blanket, pillow, fan, and sound machine. After administering the medication under the observation of a technician, you may experience an array of side effects that subside after your treatment session, including but not limited to sedation and feeling like an observer/spectator to yourself (more information in our FAQ section below).
FAQs
About SPRAVATO®
If you have tried medication and therapy to help with your depression, but none of them helped, SPRAVATO® (esketamine) nasal spray is a new depression medication and the first nasal spray medication specifically for adults with treatment-resistant depression who have tried antidepressants and augmentations but have not had success in symptom relief.
SPRAVATO® (esketamine) nasal spray is indicated for the treatment of:
- Treatment-resistant depression (TRD) in adults as monotherapy or in conjunction with an oral antidepressant.
- Depressive symptoms in adults with major depressive disorder (MDD) with acute suicidal ideation or behavior in conjunction with an oral antidepressant.
The U.S. Food & Drug Administration approved SPRAVATO® on March 5, 2019, and is only available to patients at certified treatment centers in the United States, such as Rochester Center for Behavioral Medicine (RCBM).
This treatment is approved for adults ages 18 and older.
SPRAVATO® is available only through a restricted distribution program called the SPRAVATO® REMS (Risk Evaluation and Mitigation Strategy). A REMS program is in place to ensure the safety of all patients treated with SPRAVATO®. The Rochester Center for Behavioral Medicine’s SPRAVATO® Program operates under the REMS program for service implementation at our office.
The goals of the REMS are to mitigate the risks of serious adverse outcomes resulting from sedation and dissociation caused by SPRAVATO® administration and abuse and misuse of SPRAVATO® by ensuring SPRAVATO® is only dispensed and administered to patients in medically supervised healthcare settings that monitor these patients, ensuring pharmacies and healthcare settings that dispense SPRAVATO® are REMS certified, ensuring patients are informed about serious adverse outcomes from dissociation and sedation and the need for monitoring, and enrolling all patients who receive treatment in an outpatient healthcare setting in a REMS registry to characterize the risks further and support safe use.
Share Link: About SPRAVATO®
What’s the difference between Major Depression with Suicidal Thoughts or Behavior (MDSI) and Treatment Resistant Depression (TRD) diagnosis?
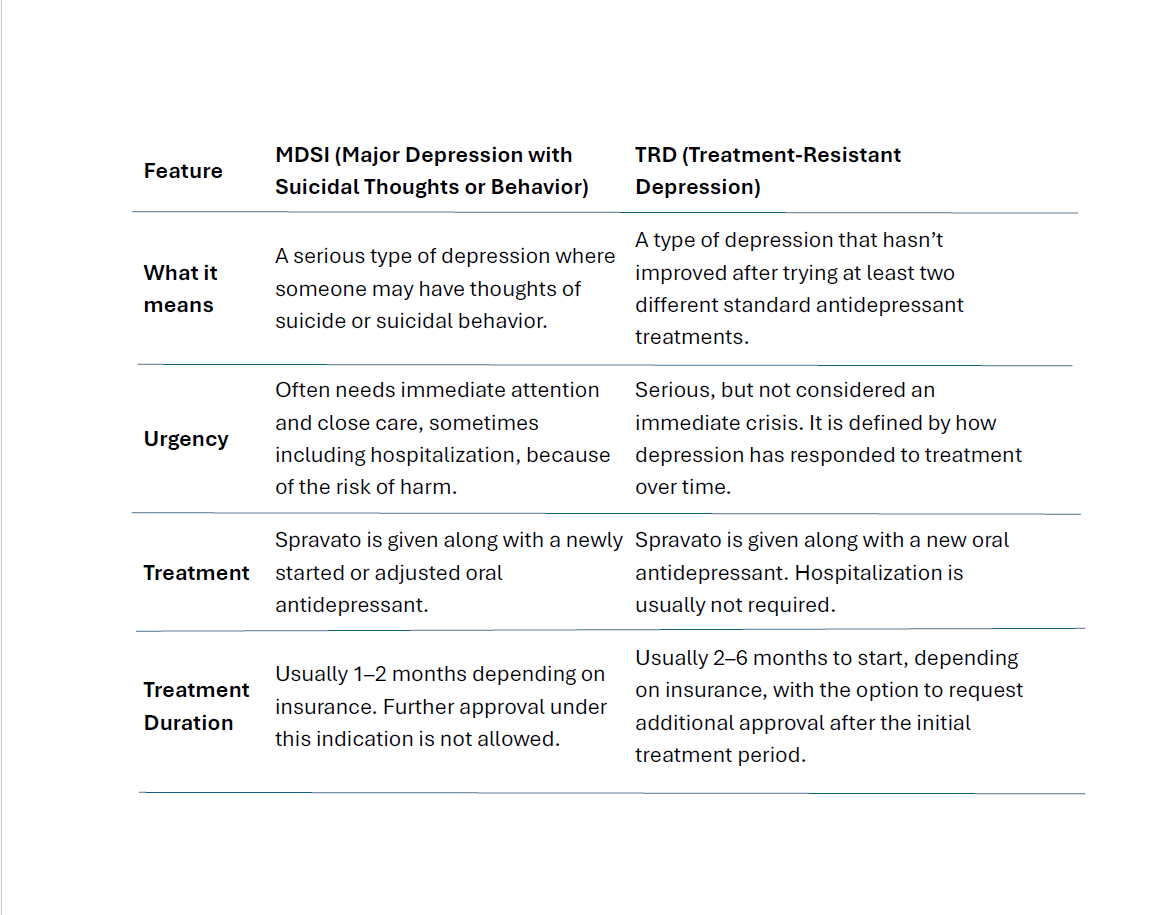
What is the difference between ketamine and esketamine (SPRAVATO®)?
Ketamine is a generic drug used off-label for depression, while SPRAVATO® is a brand-name nasal spray derived from ketamine and FDA-approved for treatment-resistant depression. While SPRAVATO® and Ketamine are chemically related, SPRAVATO® is not the same as IV Ketamine. Only SPRAVATO® has undergone extensive controlled clinical trials that informed the FDA approval of the medicine for use in adults with treatment-resistant depression and to treat depressive symptoms in adults with major depressive disorder with acute suicidal ideation or behavior.
Esketamine is made from a drug called ketamine, an anesthetic that has also been used for many years to treat depression. Because Esketamine is more potent, it can be used at a lower dose and has fewer side effects. Esketamine has earned FDA approval specifically for use as a nasal spray for those with treatment-resistant depression. Because the FDA approves it, it’s more likely that insurance companies will cover the treatment.
Mathew Perry's tragic story is now widely circulated. As a potential patient, you may have concerns. Please be aware:
- There is a difference between SPRAVATO® and esketamine. SPRAVATO®, the isomer of ketamine, has been approved by the FDA for mental health treatment. Ketamine has not been approved,
- Our post-infusion monitoring adds incredible safety to the medication.
- RCBM has years of experience with SPRAVATO®, dating back to pivotal trials. We studied this medication before it was FDA-approved.
- Our SPRAVATO® dosing is fixed, and toxic blood levels will not be exceeded.
- Mathew Perry's death reminds us of the high stakes associated with depression and treatment and the reason non-mental health experts should not be prescribing this medication.
For more information on Ketamine, please review:
Ketamine for Treatment-Resistant Depression and Related Conditions: A Review of a Novel and Needed Treatment Option by Benjamin Young, MD
Share Link: What is the difference between ketamine and esketamine (SPRAVATO®)?
Who cannot use SPRAVATO®?
You cannot use SPRAVATO® if you…
-Have a Blood Vessel Disease
-Have an abnormal connection between your blood vessels (arteriovenous malformation)
-Have a history of bleeding in the brain (intracerebral hemorrhage)
-Are allergic to Esketamine, Ketamine
-Are Lactating, Pregnant, or planning to become pregnant
-Active substance use disorder
-HIV
Precautions: If you are interested in SPRAVATO®, talk to your healthcare provider if you have the following medical conditions…
- Hypertension (High blood pressure)
- History of Stroke or Heart Attack
- Heart Valve Disease
- History of Brain Injury
- Liver Disease
- History of Psychosis
- History of Seizures
- History of Substance Abuse
- On MAO inhibitors
Share Link: Who cannot use SPRAVATO®?
Does my insurance cover SPRAVATO® treatment?
- Insurance coverage varies based on the individual health plan. We encourage you to check your insurance benefits for SPRAVATO® coverage, including co-pays and deductibles, along with whether SPRAVATO® falls under your medical or pharmacy benefits. The RCBM SPRAVATO® Program does not participate with TriCare, Carelon Behavioral Health, UMR, Beaumont UMR, Blue Care Network, Humana, and Medicaid. If you have one of these health plans, please visit SPRAVATO®.com to find a SPRAVATO® center that takes your insurance.
- All insurances require pre-authorization and continued authorization for SPRAVATO® treatment, while each insurance company has different criteria for authorization of SPRAVATO®. This includes a history of inadequate response to several different classes of anti-depressant medications with a trial of a minimum of 8 - 12 weeks each, along with augmentation strategies.
- Your healthcare provider must refer you for SPRAVATO® treatment and document the medical necessity of SPRAVATO® based on the required criteria.
- If you have a commercial health plan, SPRAVATO with me is available to help you navigate access and affordability.
Share Link: Does my insurance cover SPRAVATO® treatment?
How effective is SPRAVATO® treatment?
In clinical studies, patients who achieved stable remission with SPRAVATO® augmented with an antidepressant showed a 51% decrease in risk of relapse*. In addition, there was a 70% risk reduction for depressive symptoms among those who achieved a stable response compared to an antidepressant alone.
For individuals with TRD
In clinical studies, improvement of depressive symptoms was demonstrated at four weeks by SPRAVATO® plus an oral antidepressant, compared with placebo nasal spray plus an oral antidepressant. Not all patients will respond to SPRAVATO®.
For individuals with MDSI
In clinical studies, those who took SPRAVATO® and an oral antidepressant experienced a greater reduction of depressive symptoms at 24 hours compared to those who took a placebo plus an oral antidepressant. Further reductions were seen consistently through four weeks (25 days) of treatment, so it is essential to follow the treatment plan that you and your healthcare provider have made. Not all patients will respond to SPRAVATO®.
*As of February 2025, the FDA has approved Spravato as monotherapy for adults living with treatment-resistant depression (TRD).
Share Link: How effective is SPRAVATO® treatment?
How does RCBM’s SPRAVATO® Treatment Resistant Depression Clinic stand apart from other programs?
RCBM provides a welcoming and comfortable atmosphere so patients can relax and engage in their treatment. Our staff is highly professional and well-trained. Unlike other centers, our program offers many amenities and services.
Amenities:
- Blankets
- Call buttons for assistance when the technician or medical provider is not present in the room
- Fans and heaters
- Handicap access
- On-site parking
- Pillows
- Power Outlets
- Private treatment rooms
- Recliners
- Snacks and beverages for nausea
- SPRAVATO® playlists on Spotify
- Television in each treatment room
- Waiting Areas for Caregivers
- Wi-Fi
Services:
- Appointment Scheduling
- Appropriate and accurate clinical documentation to ensure continued insurance authorizations so as not to interrupt your treatment
- Communication and coordination of care with your internal and external provider from referral to continued treatment
- Insurance Verification
- Well-trained and attentive staff
Share Link: How does RCBM’s SPRAVATO® Treatment Resistant Depression Clinic stand apart from other programs?
What are common patient questions and answers about SPRAVATO® treatment?
When am I going to begin feeling better? How do I know if it’s working for me?
Patients typically start feeling the benefits of SPRAVATO® around week 8, but the timing can vary from patient to patient. It's important to emphasize that, like oral antidepressants, SPRAVATO® may not be effective for every patient. Patients are encouraged to keep a journal of their feelings during and between SPRAVATO® treatments to assess its effectiveness. This journal can be used to discuss treatment efficacy during follow-up appointments.
How long am I going to have to be treated?
The average length of treatment nationwide is two years. However, each patient's duration is unique and depends on their progress with the medication. The duration is determined based on conversations between the patient and the provider, taking into account the medication's effectiveness and the patient’s ability to maintain a consistent schedule.
How long until I can stop taking additional medications for my depression?
When referring someone for SPRAVATO®, it's important to understand that it is not a cure or a stand-alone medication. It is meant to complement an oral anti-depressant and help with symptom relief. While remission may be possible, it is not guaranteed.
What am I supposed to do during the appointments?
There are no required activities to be done during SPRAVATO®. The only requirement is to administer the medication in order to receive its benefits. However, engaging in activities such as listening to guided therapy/meditation sessions or SPRAVATO® playlists on Spotify may provide additional benefits.
Share Link: What are common patient questions and answers about SPRAVATO® treatment?
Ready to get started? SPRAVATO® referral and evaluation timeline
The following is a timeline of what you should expect from referral through the course of treatment:


Share Link: Ready to get started? SPRAVATO® referral and evaluation timeline
Please read our Full Information SPRAVATO® Pamphlet before submitting a patient interest or Healthcare provider referral form.
Patients must have an active diagnosis of either Treatment Resistant Depression (TRD) or Major Depression with Acute Suicidal Ideation (MDSI) in order to be eligible for treatment with SPRAVATO®.
For more information on SPRAVATO®
Please note the important requirements for treatment in our program before completing the interest form or referral forms:
- Patients must have an active diagnosis of either Treatment Resistant Depression (TRD) or Major Depression with Acute Suicidal Ideation (MDSI) to be eligible for treatment with Spravato.
- Business hours are between 9:00 am – 5:00 pm, with the last treatment appointment scheduled at 3:00 pm.
- Appointments are at least two hours long and require a twice-weekly regimen for the first four weeks, followed by once weekly for one month. Dosing is continued based on response to treatment.
- Patients must have a driver to and from each appointment and are not allowed to resume driving until the next morning.
Watch: Expert Insights on Spravato® Treatment Resistant Depression Clinic
Spravato Program at RCBM
Dr. Joel Young discusses the use of Spravato for treatment-resistant depression and how to enroll in our Spravato Program at RCBM.
The Spravato Program at RCBM
Hailee Mika, Spravato Program Coordinator, discusses Spravato and how it helps treatment-resistant depression. She also explains how our program works at RCBM, from referral and authorization to the treatment experience. Note: As of February 2025, the FDA has approved Spravato as monotherapy for adults living with treatment-resistant depression (TRD).
The Spravato Program Referral Process
Hailee Mika, Spravato Program Coordinator, explains how Spravato works for treatment-resistant depression and how to refer patients to the Spravato Program at RCBM. Note: As of February 2025, the FDA has approved Spravato as monotherapy for adults living with treatment-resistant depression (TRD).
The Spravato Program Treatment Experience at RCBM
Hailee Mika, Spravato Program Coordinator, discusses your experience in our Spravato Program and eligibility requirements.Substance Abuse & Addiction Program

Our Substance Abuse Dependency Program has been established to help the care of individuals struggling with addiction and the abuse of opiates, benzodiazepines, and alcohol. We are dedicated to helping those patients who have exhausted all options of treatment and are seeking help to recovery. RCBM offers a unique approach to work with these individuals because we understand that addiction is a disease and with the right tools and support, we can help patients find solutions. Our primary goals for treatment include:
- Tapering off to Opiate-free by the end of treatment
- Minimizing the use of benzodiazepines
Joel Young, MD and Aliya Pasik, PA-C oversee the Substance Abuse Dependency Program initiative at RCBM. Our team has a specialized background in the treatment and care of those suffering from addiction and abuse. RCBM is very dedicated to treating substance abuse disorders and mental illness and feels that giving someone the gift of sobriety is one of the greatest gifts you can give a person struggling with chronic addiction. Establishing a trusting relationship with patients is our priority at RCBM. Establishing a personalized treatment plan involves four steps.
The first step in the Substance Abuse Dependency Program is to make an appointment with one of the members of our team. At that first appointment, the patient will explain the details of the substance abuse and addiction that brings them to RCBM seeking help.
At the second step, the patient will be scheduled for a psychological evaluation and screening. This will provide a better indication of the presenting issues along with any historical information.
The third step involves results from the psychological screening and analysis of the data in order to develop a personalized treatment plan. Depending on the type of substance abuse, specific medications will be prescribed for treatment, which may include:
- Suboxone --a medication for the treatment of opioid dependence
- Antabuse -- a powerful deterrent to drinking
- Vivitrol -- a new injectable medication with 30 days of coverage
- Campral - to help control cravings
 The fourth and final step includes referral and coordination of care with one of our certified advanced alcohol and drug counselors who will also be involved in the patient's care. Dr. Young and Aliya will also determine an appropriate schedule for medication management and will consult with the patient’s primary care physician (PCP) regarding the treatment plan.
The fourth and final step includes referral and coordination of care with one of our certified advanced alcohol and drug counselors who will also be involved in the patient's care. Dr. Young and Aliya will also determine an appropriate schedule for medication management and will consult with the patient’s primary care physician (PCP) regarding the treatment plan.
Prior to every visit, we will run a MAPS (Michigan Automated Prescription System) to make sure patients are not receiving opiates or benzodiazepines from another provider. The safety of our patients is of utmost importance.
Our comprehensive program will give patients the structure and support they need to find a treatment option that is customized to their addiction. Take control of the addiction. Do not wait for the legal system to take control of it.
Program Director of Addiction Medicine
Watch: Expert Insights on Substance Abuse & Addiction Program
Addiction Treatment
Aliya Pasik, PA-C, Program Director, Addiction Recovery Clinic discusses the RCBM Addiction Medicine Program at RCBM.
Addiction and Relapse Prevention During COVID-19
Whenever there's a time of high stress, the risk of relapse or the risk of escalating use is increased. Judy Redmond, MA, LPC, LLP, CAADC and Aliya Pasik, PA-C discuss relapse prevention during COVID-19.
Addiction, Signs and Recovery | with Aliya Pasik, MS, PA-C
Aliya Pasik, MS, PA-C, is the Program Director of the Addiction Recovery Center at the Rochester Center for Behavioral Medicine. Aliya addresses the many forms of addiction and substance abuse, particularly as it relates to the 50+ demographic. She describes underlying conditions that lead to self-medication such as ADHD, loneliness, anxiety, depression, and boredom. Alcohol abuse seems to be on the rise, especially during the Coronavirus pandemic. Aliya also discusses specific clinical programs that she is spearheading, describes certain signs that lead to substance abuse, and provides medical, cognitive, and holistic ways for patients and their families to have conversations that lead to recovery.
Therapy and Addiction Recovery
David Price, LPC, CAADC discusses therapy as a central and transformative role in supporting someone through addiction. He explains that therapy helps patients safely explore psychological, emotional and behavioral patterns that drive their substance use. David uses strategies including CBT that looks at patterns, triggers and thoughts; relapse prevention planning for high risk situations and urges to delay impulses; motivational interviewing and stages of change.
Book Review - The Sobriety Manual by Aliya Pasik, PA-C
In her new book, Aliya Pasik, PA-C, explains various types of addictions and their consequences in easy-to-understand terms, as she guides you on how to get the help you need. Don’t wait for the legal system to make treatment mandatory. Addictions are life-threatening concerns, and this new book, The Sobriety Manual: The essential tool for sobriety, health, and happiness, is your companion on your recovery journey. Read more here: https://www.rcbm.net/behavioral-medicine/the-sobriety-manual/
Relapse Prevention Treatment
Judy Redmond, LPC, LLP, CAADC explains common triggers for relapse and that thoughts and urges are a normal part of recovery. She discusses the importance of noticing and using tools for long term sobriety such as building self awareness, understanding triggers, and treating underlying mental health issues such as anxiety, depression and ADHD. Being part of a recovery community can offer support to stay on track for long term sobriety.Telemedicine

We are pleased to offer HIPAA-secure video sessions for medication management, psychotherapy, and medical nutrition therapy. We intend to provide telehealth services as a permanent offering.
To keep our patients and staff safe, RCBM transitioned to telehealth during COVID-19. Our patients have expressed high levels of satisfaction with their telehealth experience, and a body of evidence supports this modality for children, adolescents, and adults.
RCBM uses the HIPAA secure platform called Zoom, which is now integrated into our Electronic Medical Record system, allowing for ease of scheduling and appointment reminders. Check your e-mail before your scheduled appointment for your Zoom link and other logistical details. The benefits of telemedicine include ease, convenience, privacy, and access, along with increased choice and options. This service fits into your lifestyle rather than the other way around. Most major insurance plans now have coverage for telehealth. Please check with your plan to confirm that you have this benefit.
The COVID pandemic has demanded innovation and flexibility from all of us. Since the start of the pandemic, RCBM has used telehealth to support the mental health needs of patients throughout Michigan. We found that we could safely meet and serve Michiganders from Monroe to Marquette. Regulations may change once the Public Health Emergency is lifted. RCBM will fulfill all regulatory obligations. We are committed to telehealth and will work to make these changes permanent.
Our patients are so very pleased with telehealth services!
"Great professionals here! It's so nice to talk with someone from the comfort of your own home. We trust them with our entire family."“I was skeptical about telehealth at first, as therapy sessions are so personal. Within a few moments of speaking with my therapist, I forgot that we were on Zoom.”
“I used to have to take 2 hours out of my day to drive to my appointment, wait in the waiting room, have my appointment, and then go back to work. I can now have my session and be back to work within an hour. Telehealth has been a huge convenience for me!”
“Honestly I felt so comfortable and welcomed, also nice to feel validated as well as talking about what/how I should do differently. Very nice Tele-visit and I feel very motivated to become better.”
Watch: Expert Insights on Telemedicine

RCBM and Telehealth
Melissa Oleshansky, PhD, LP, RYT shares how telehealth services work at RCBM and why they are so valuable. It allows us to fit confidential care into our busy lives as travel to appointments is not needed. We offer telehealth for medication management, psychotherapy and medical nutrition therapy services.Transcranial Magnetic Stimulation (TMS)

Repetitive Transcranial Magnetic Stimulation (rTMS) is an innovative, FDA-cleared treatment that offers new hope for people living with depression. Designed for adults and adolescents, ages 15 and up, who haven’t found relief with medication alone, rTMS is a non-invasive therapy that targets the root of depression—brain activity—without surgery, sedation, or downtime.
Using gentle magnetic pulses, rTMS stimulates specific areas of the brain involved in mood regulation, helping restore healthier neural connections over time. Treatments are performed in a comfortable outpatient setting, typically last under 30 minutes, and allow you to return to your day immediately afterward.
With minimal side effects and strong clinical evidence supporting its effectiveness, rTMS offers a powerful alternative for those seeking lasting relief and improved quality of life. If depression has been holding you back, rTMS may be the breakthrough you’ve been waiting for.
LEARN MORE ABOUT NEUROSTAR rTMS
Understanding SPRAVATO® vs TMS
How rTMS works
During treatment, a small magnetic coil is placed on your scalp. The coil delivers brief magnetic pulses to targeted areas of the brain that may not be working as effectively. These pulses help “wake up” brain cells and improve communication between them, which can lead to better mood and symptom relief over time.
- You are awake and comfortable during treatment
- Sessions typically last 30–40 minutes and are available from 9:00am to 3:30pm Monday to Friday
- The first visit is called a ‘mapping’ visit and lasts one hour, where we find the treatment location for each patient, with these sessions available Monday and Tuesdays at 4:00pm only
- No sedation or recovery time needed
- You can drive yourself home and return to daily activities right away
- Treatments are daily for 6 weeks with a tapering schedule for 3 weeks after
Who may benefit from rTMS
rTMS is most often used for adults or adolescents with depression (MDD), without suicidal ideation, who have not found enough relief from antidepressant medications and for adults with obsessive-compulsive disorder (OCD).
Benefits of rTMS
- No medication-related side effects like weight gain or fatigue
- Non-invasive and well-tolerated
- FDA-cleared and supported by extensive clinical research
- Can be effective when other treatments haven’t worked
Safety and side effects
rTMS is considered very safe. Some people experience mild scalp discomfort or headaches at the beginning of treatment, which usually improve after the first few sessions. Serious side effects are rare.
A personalized approach to care
At RCBM, we use NeuroStar® Advanced Therapy, which is the #1 physician-recommended rTMS treatment. NeuroStar® is the only treatment clinically proven to be effective through 12 months in patients with treatment-resistant depression (TRD). In addition, OCD treated with rTMS has shown to improve OCD symptoms.
- In adults, 83% showed improvement in depressive symptoms, and 62% achieved symptom relief (remission).
- In adolescents, 78% of patients showed improvement in depressive symptoms, and 48% achieved symptom relief (remission).
- A total of 57.9% of patients showed a greater than 30% reduction in the severity of OCD symptoms, and 52.4% experienced a sustained response.
Your treatment plan is tailored to your symptoms, history, and treatment response. Our team works closely with you every step of the way to ensure comfort, safety, and the best possible outcomes.
FAQs
Who is a good candidate for rTMS?
A good candidate for Transcranial Magnetic Stimulation (rTMS) is typically someone who meets several of the criteria below.
You may be a good candidate for rTMS if you:
✔ Have major depressive disorder (MDD) or obsessive compulsive disorder (OCD)
rTMS is FDA-cleared for 15 -75 year olds with either MDD or OCD, especially when symptoms are moderate to severe.
✔ Have not had enough relief from antidepressant medications
Many people who pursue rTMS have tried two or more antidepressants without adequate improvement or have had side effects that made medications hard to tolerate.
✔ Are looking for a non-medication treatment option
rTMS does not involve daily medication, sedation, or anesthesia.
✔ Can attend regular treatment sessions
rTMS is usually given 5 days per week for 6 weeks, so the ability to attend scheduled visits is important.
rTMS may also be appropriate if you:
- Are hoping to avoid potential medication side effects like weight gain, fatigue, or sexual dysfunction
- Want to stay alert and resume normal activities immediately after treatment
- Have depression with anxiety symptoms (many patients experience improvement in both)
Who may not be a good candidate?
rTMS may not be recommended for individuals who:
- Have a history of seizure disorder
- Have certain implanted medical devices or metal in the head, including cochlear implants
- Are unable to sit comfortably for treatment sessions
Share Link: Who is a good candidate for rTMS?
What is the difference between TMS and rTMS?
Transcranial Magnetic Stimulation (TMS) is the umbrella term for a non-invasive treatment that uses magnetic pulses to stimulate specific areas of the brain. rTMS stands for Repetitive Transcranial Magnetic Stimulation and is a specific type of TMS that uses repeated pulses. It is the most common type of TMS used in clinical practice.
Share Link: What is the difference between TMS and rTMS?
Does my insurance cover rTMS?
- Insurance coverage varies by individual health plan. We encourage you to check your insurance benefits for TMS coverage, including co-pays and deductibles. The RCBM TMS Program does not participate with TriCare, Carelon Behavioral Health, UMR, Beaumont UMR, Blue Care Network, Humana, or Medicaid. If you have one of these health plans, please visit NeuroStar to find an rTMS center that takes your insurance.
- All insurance plans require pre-authorization and ongoing authorization for TMS treatment, and each insurer has different authorization criteria. This includes a history of inadequate response to a stipulated number of classes of antidepressant medications or medications for OCD by your insurance company, with a trial of a minimum of 4 - 8 weeks each, along with augmentation strategies such as psychotherapy based on your specific insurance company criteria.
- Your psychiatrist must refer you for rTMS treatment and document the medical necessity of rTMS in accordance with the required criteria.
Share Link: Does my insurance cover rTMS?
What are common patient questions and answers about rTMS treatment?
How does rTMS work?
Certain parts of your brain help control your mood. When the connections in these areas aren’t working as well as they should, communication between brain cells slows down, which can lead to depression. rTMS helps reactivate these connections, allowing the brain to communicate more normally again.
What is involved in the initial mapping session of my rTMS treatment?
An rTMS mapping session is an appointment that helps your care team find the exact spot on your head to treat—and the right treatment strength for you.
During the session, you’ll sit comfortably in a chair while a small magnetic coil is placed against your scalp. The provider sends brief magnetic pulses and watches for a small movement in your hand or fingers. This movement allows them to observe how your brain responds and helps determine the minimum stimulation required to work safely and effectively.
Using this information, they carefully measure and mark the treatment location on your head so each session is consistent. The mapping session is not painful, does not involve needles or surgery, and usually takes 30 - 45 minutes, followed by your first treatment session, which takes 20-30 minutes. It’s an important step to personalize your rTMS treatment and make sure it’s both safe and effective.
Do I still take my psychotropic medications during rTMS treatment?
There are some medications that are contraindicated with TMS. However, for any medications that are not contraindicated, you will continue to take them as prescribed.
When will I start to feel better?
Individuals' experiences with NeuroStar® rTMS vary. The timing of when you feel improvement in your depressive symptoms may not be the same as that of other individuals. Some individuals may begin to experience positive effects within the first week, whereas others may not notice them until the end. It is important to trust the process and stay committed to all 36 treatments. Some of the positive changes include increased energy, improved sleep quality, elevated mood, better concentration, improved eating habits, restored interest in hobbies, and improved social disposition.
Share Link: What are common patient questions and answers about rTMS treatment?
Ready to get started? rTMS referral and evaluation timeline
As this is a new program at RCBM, we will process referrals in the order received. Thank you
TMS Department Contact Information:
Email: tms@rcbm.net
Phone: (586) 684-1915
Fax: (947) 230-0565
Share Link: Ready to get started? rTMS referral and evaluation timelineWatch this video to learn about Bart's story with NeuroStar rTMS treatment
Patients must have an active diagnosis of Major Depressive Disorder (adults or adolescents) or patients must have an active diagnosis of Obsessive Compulsive Disorder (adults) in order to be eligible for rTMS treatment.
Please read our TMS Adult or Adolescent Patient Brochure before submitting a Patient Interest or Healthcare Provider Referral form.
NeuroStar® Adult Patient Brochure Depression
NeuroStar® Adolescent Patient Brochure Depression
NeuroStar® Adult Patient Brochure OCD
Please note the important requirements for treatment in our program before completing the interest form or referral forms:
- Patients must have an active diagnosis of either major depressive disorder (MDD) or obsessive-compulsive disorder (OCD) for TMS treatment.
- Business hours are 9:00 am to 3:30 pm, except for Mapping visits, which are scheduled only on Mondays and Tuesdays at 4:00 pm.
- Appointments are 30 - 40 minutes long and require a 5-day per week regimen for 6 weeks
- The initial mapping session, followed by treatment, lasts one hour.
Patient Interest Form for rTMS Treatment:
For patients who have been seen by an RCBM provider within the past 6 months, please DO NOT complete the forms below. Please discuss your interest with your RCBM provider at your next appointment. Thank you!
If you are a New Patient to RCBM, please visit the “New Patient” link, also located on the navigation bar at the top of the page, and complete registration. On the registration form, you will select that you have an interest in rTMS.
Healthcare Professional Referral Form for rTMS Treatment:
Please read the information above. If you have any additional questions or concerns before completing the respective interest form, please email tms@rcbm.net.
Watch: Expert Insights on Transcranial Magnetic Stimulation (TMS)

What is TMS?
Joel Young, MD, Medical Director and Founder of RCBM explains how Transcranial Magnetic Stimulation (TMS) works and what to expect from treatment.
TMS at RCBM
Joel Young, MD, Medical Director and Founder discusses the Transcranial Magnetic Stimulation (TMS) program at RCBM and how it works along with who is a good candidate.
What to expect about the TMS Program
Oriol Paricio Sunyer, BS, TMS Program Coordinator explains how the Transcranial Magnetic Stimulation (TMS) program works at RCBM and what to expect when the patient is referred to the program.
What to expect during a TMS visit
Oriol Paricio Sunyer, BS, TMS Program Coordinator conveys what to expect during a Transcranial Magnetic Stimulation (TMS) visit. He describes the initial mapping appointment followed by the treatment sessions.Trauma Treatment
Traumatic experiences can occur when there is an emotional disturbance or response from an event(s) or circumstance(s) that was perceived as life-threatening or harmful physically or mentally. Some traumatic experiences may include but are not limited to being in active combat in the military, experiencing violence or abuse, being in an auto accident, having a grave illness, being in a natural disaster, or experiencing a mass shooting, which can result in PTSD.
When experiencing trauma, the individual may be flooded with strong emotions, and consequently, the brain may not process, organize, and store the information in the usual way.
Post-Traumatic Stress Disorder (PTSD) is one outcome of trauma. It is an anxiety disorder that occurs after an individual has personally experienced or witnessed a violent event such as a natural disaster, mass violence, active combat, working as a first responder, sexual trauma, or domestic abuse.
FAQs
What is trauma?
Trauma can occur when an individual experiences a life-threatening event or witnesses someone else’s life-threatening event. Some examples of traumatic events are:
- Active combat
- Physical, emotional, and sexual abuse
- Serious accidents
- Grave illnesses
- Natural disasters
- Terrorist attacks
- Mass shootings
- Relationship traumas include childhood abandonment, being abused in childhood, or being bullied.
What is Post-Traumatic Stress Disorder (PTSD)?
After a traumatic or upsetting experience, many people experience a change in mood, problems sleeping or suffer from recurring memories of the event. This can make it difficult to manage life in the way they did before the trauma, and it can interfere with work, school, and interacting with family and friends. This is normal and often improves over several months. Sometimes, people find that these symptoms do not go away alone. When that happens, it is important to reach out to a mental health provider who can evaluate and treat PTSD.
Read more information on PTSD and view videos on the U.S. Department of Veterans Affairs website
Share Link: What is trauma?
What effects can traumatic events have on an individual?
Traumatic events can cause lasting psychological symptoms, including the following from the National Institute for Mental Health:
Re-experiencing symptoms
- Flashbacks—reliving the trauma over and over, including physical symptoms such as:
- Racing heart or sweating
- Nightmares
- Intrusive thoughts or fragments of memories of the trauma
Avoidance symptoms
- Staying away from places, events, or objects that are reminders of the experience
- Feeling emotionally numb Feeling strong guilt, depression, or worry
- Losing interest in activities that were enjoyable in the past
- Having trouble remembering the dangerous event
Events that remind a person of the traumatic event can trigger avoidance symptoms. These symptoms may cause a person to change his or her personal routine. For example, a person who usually drives may avoid driving or riding in a car after a bad car accident.
Hyperarousal symptoms
- Easily startled
- Feeling tense or “on edge”
- Difficulty sleeping and/or having angry outbursts
Hyperarousal symptoms may make it hard to do daily tasks, such as sleeping, eating, or concentrating.
Share Link: What effects can traumatic events have on an individual?
How is trauma treated at RCBM?
Not everyone who experiences trauma goes on to develop PTSD, but for those who do, there is an effective treatment that can alleviate or reduce the intensity of symptoms. At the Rochester Center for Behavioral Medicine, we offer a range of treatments for trauma. These include cognitive behavioral therapy, EMDR, polyvagal therapy, and medication management.
At the Rochester Center for Behavioral Medicine, PTSD is treated with a combination of cognitive-behavioral therapy (CBT) and, when necessary, medications. This effective approach can help individuals with PTSD identify situations that trigger their “fight or flight” response. Using the cognitive-behavioral techniques of flooding and systematic desensitization, the therapist and patient can work together to safely reintroduce situations that have become too anxiety-provoking for the patient. Over time, irritability, flashbacks, and nightmares subside, the patient can return to their pre-trauma functionality, and long-term success is within reach.
Trauma-focused CBT (TF-CBT) is an evidence-based treatment specifically for children and adolescents impacted by trauma and their parents or caregivers. It is a components-based treatment model that incorporates trauma-sensitive interventions with cognitive behavioral, family, and humanistic principles and techniques. TF-CBT has proved successful with children and adolescents (ages 3 to 18) who have significant emotional problems (e.g., symptoms of posttraumatic stress disorder, fear, anxiety, or depression) related to traumatic life events. It can be used with children and adolescents who have experienced a single trauma or multiple traumas in their lives.
Eye Movement Desensitization and Reprocessing (EMDR) is a treatment modality that has been helpful to people who are suffering from the effects of trauma. After encountering a traumatic event, such as an auto accident, domestic abuse, violence, or perinatal loss, fragmented memories may intrude into daily life. This can result in feelings of helplessness or low self-esteem. Sometimes, individuals turn to alcohol or substance abuse to decrease the intrusive memories. EMDR allows the traumatic event to be fully processed so the individual is freed from re-experiencing the event in everyday life. This may result in a better quality of life and hope and well-being. It is also used in conjunction with traditional therapy.
Share Link: How is trauma treated at RCBM?
What is trauma focused cognitive behavioral therapy (TF-CBT)?
Generally, TF-CBT is completed in 12-18 weeks as it is very structured. The clinician works with the child directly, as well as conducts parent sessions to review the information processed with the child with the parent so that the parent can help the child practice the coping skills between sessions and develop a common language for them to speak about the trauma. After the child and parent receive psychoeducation regarding the trauma itself, the child is taught relaxation skills to utilize when managing the strong reactions they may have to trauma triggers or for general anxiety. Once the stress coping mechanisms are in place, the trauma specialist will work with the child on affect regulation: understanding and managing emotions. The relaxation skills and affect regulation skills tend to help bring some relief from the day to day symptoms of trauma, however more work is needed. The clinician then moves into what is called "cognitive coping," essentially helping rewrite negative and maladaptive thoughts related to the trauma. A large portion of the treatment is utilized to help the child work on their "trauma narrative," telling and retelling their story. In the process, the clinician helps the child utilize some aspects of relaxation, affect regulation, and cognitive coping to work through the stress that arises when the child recounts the trauma. Once the narrative is ready, the child shares the trauma narrative with a caregiver or supportive person, most typically a parent or guardian. The clinician has prepared the parent/guardian/support person before sharing the narrative so that all that person should do is listen and provide support to the child without adverse reactions or arguing about the details. The final steps of TF-CBT are in-vivo exposure (whenever possible), helping the child make sense of the trauma, and working to ensure future safety.
Share Link: What is trauma focused cognitive behavioral therapy (TF-CBT)?
What is Eye Movement Desensitization and Reprocessing (EMDR)?
When experiencing trauma, the individual is flooded with strong emotions, and consequently, the brain cannot process, organize, and store the information in the usual way. EMDR allows the traumatic event to be fully processed, so the individual is freed from re-experiencing the event in everyday life. This may result in a better quality of life and hope and well-being.
Eye Movement Desensitization and Reprocessing (EMDR) is a treatment modality that has been helpful to people who are suffering from the effects of trauma. After encountering a traumatic event, such as an auto accident, domestic abuse, violence, perinatal loss, or others, fragmented memories may intrude into daily life. This can result in feelings of helplessness or low self-esteem. Sometimes, individuals turn to alcohol or substance abuse to decrease the intrusive memories.
According to EMDRIA, EMDR is an evidence-based, extensively researched, and widely recognized effective trauma treatment therapy in guidelines published by the International Society for Traumatic Stress Studies, the World Health Organization, and a growing number of national and international organizations. Treatment guidelines are based on reviews that evaluate the research of established evidence-based mental health treatments.
All of RCBM’s EMDR therapists have completed EMDRIA-approved training.
Share Link: What is Eye Movement Desensitization and Reprocessing (EMDR)?
Who is EMDR specifically for at RCBM?
EMDR focuses on a specific event, memory, or physical sensation related to that event/memory. In situations of panic/phobia, perceived or upcoming events that cause feelings of anxiety can be treated. Rating scales are used upon assessment.
Who is EMDR for at RCBM?
- Anxiety, panic attacks, and phobias
- Acute stress disorder
- Recent trauma
- Patients who are stabilized on their medication regimen
- Stabilized depression
- Grief and loss
- Post-traumatic stress disorder (PTSD)
- Sexual assault
- Substance abuse and addiction
- Violence and abuse
- Survivors of violence and accidents
Who Does NOT Qualify for EMDR at RCBM:
- Current or recent suicidal ideation
- Severe depression
- Anorexia nervosa
- Chronic pain that limits or inhibits eye movements/tapping
- Psychosis
- Current mania
- Recent medication change
- Recent hospitalization
Share Link: Who is EMDR specifically for at RCBM?
How do I get started in the trauma program at RCBM?
If you are a current patient at RCBM, please discuss with your clinician about treatment options at RCBM and how you can include trauma therapy in your treatment plan. If you are new to RCBM, you can initiate the admission process by completing a new patient registration form. Once you submit the form, we will match you with one of our qualified therapists specializing in trauma. Please keep in mind that you must be a resident of Michigan and willing to visit the office if needed. We are dedicated to supporting your mental health journey and look forward to working with you.
Share Link: How do I get started in the trauma program at RCBM?
Watch: Expert Insights on Trauma Treatment

Eye movement desensitization and reprocessing (EMDR) therapy
Judy Redmond, LPC, LLP, CAADC specializes in and discusses EMDR, a highly effective and efficient treatment for trauma and a broad array of other mental health challenges.
What is Trauma-Focused Cognitive Behavioral Therapy?
Olivia Nash, MA, LPC, NCC, discusses trauma-focused cognitive behavioral therapy (TF-CBT), which is designed for children and adolescents who have experienced trauma, as well as their parents or caregivers. This therapy can be utilized for those who have undergone a single traumatic event or multiple traumas in their lives.
Trauma and Informed Care
Alli Smith, LMSW discusses sexual trauma impacts mental health and daily functioning. She also conveys how underlying trauma manifests into other mental health issues. Alli explains how trained trauma therapists work with patients.Meet the Providers Who Offer Care for Trauma Treatment
Alli Smith, LMSW, CCTP
Read More
Amy Karwowski, LMSW
Read More
Judith C. Redmond, LPC, LLP, CAADC
Read More
Julie Staples MA, LPC NCC
Read More
Matthew Barsenas, LMSW, JD
Read More
Olivia Nash, MA, LPC, NCC
Read More
Sydney Salloum, LPC
Read More
Related Titles from the RCBM Reading and App list:
The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma - By Bessel Van Der KolkTransforming the Living Legacy of Trauma - By Janina Fisher
Waking the Tiger: Healing Trauma - By Peter A. Levine
PTSD Coach
Trichotillomania

Trichotillomania is a disorder characterized by the pulling of hair for non-cosmetic purposes, which can often result in significant hair loss. Hair is typically pulled from eyebrows, eyelashes, scalp, beard and pubic area, though hair from other parts of the body may also be pulled.
Individuals with Trichotillomania may also play with, bite, nibble or chew the hair. If ingested, this may cause a serious condition in need of medical attention. It is not uncommon for people with this disorder to engage in other damaging behaviors such as nail-biting or skin-picking. It appears that significant emotional experiences or feelings can trigger hair pulling. Anxiety, depression, stress, anger, and tension may increase the urge to pull. However, hair pulling may also occur when the individual is inactive and subdued; while reading, watching television, doing homework or even lying in bed.
At RCBM, we fully evaluate individuals suffering from Trichotillomania to assess the disorder and determine if any conditions result from or contribute to the pulling of hair. In addition, we assess the impact on social functioning, academic environment, and family relationships. Often, we work with the family utilizing a cognitive-behavioral approach. This consists of developing a treatment plan focusing on triggers associated with the pulling, thoughts and feelings, along with the situations where pulling occurs. We meet with the patient and family regularly to determine progress and discuss the factors contributing to the pulling/picking behaviors. It is not uncommon for clinicians to ask patients with Trichotillomania to complete activities outside of the therapy session, such as journal writing, progress calendars, worksheets, and creating barriers such as wearing band-aids/gloves or hats/scarves.
Weight Management Program

RCBM is pleased to introduce Medabolic, a medically supervised lifestyle management program that uses a multi-disciplinary, collaborative, and evidence-based approach under the medical leadership of Joel L. Young, MD, and Derek Susalla, PA-C. We address weight concerns from a risk factor reduction perspective rather than an aesthetic one.
Participation in the Medabolic program starts with an intake interview and diagnostic assessment. If the program's criteria are met, a carefully tailored treatment plan will be created based on the individual's needs, integrating the services of our highly trained team of medical providers (psychiatrists, physician assistants, and nurse practitioners), psychotherapists, and registered dietitians.
We know from thirty years of practice that overweight and obesity can cause or be caused by mental health symptoms. RCBM offers the psychological and psychiatric components that are often missing from most programs that address weight-related concerns.
For current and prospective patients who are interested in and qualify for GLP-1 medications but cannot obtain insurance coverage, we can offer private-pay rates for Wegovy and Zepbound through the manufacturer. We also offer generic and affordable alternative weight management medications that may be covered by your insurance. Note: Now approved: A new once-daily pill for weight management, Wegovy® tablet. Learn more about various medications offered for weight loss in the FAQs below.
What is the Medabolic Program?
Medabolic is RCBM’s personalized weight loss program in Michigan. Built on a collaborative, evidence-based model, Medabolic focuses on reducing health risks. Under the care of Dr. Joel Young and Derek Susalla, PA-C, patients receive a personalized plan that may include medical providers, therapists, and dietitians - all working together to reduce health risks, not just focus on appearance.
We integrate medical, psychological, and nutritional care to help you:
- Manage weight effectively
- Improve energy and mood
- Stabilize metabolism and blood sugar
- Build sustainable habits for long-term wellness
In a randomized clinical trial that included 611 adults with overweight or obesity, 68 weeks’ treatment with once-weekly subcutaneous semaglutide vs placebo, combined with intensive behavioral therapy (and a low-calorie diet for the initial 8 weeks), resulted in reductions in body weight of 16.0% vs 5.7%, respectively. This difference was statistically significant, emphasizing the importance of a multidisciplinary team in treating obesity. Therefore, when used as an adjunct to intensive behavioral therapy and an initial low-calorie diet, once-weekly subcutaneous semaglutide produced significantly greater weight loss than placebo during 68 weeks in adults with overweight or obesity.
How It Works
Every patient starts with a comprehensive intake and diagnostic assessment. Based on your needs, our team builds a customized treatment plan that includes:
- Psychiatric evaluation and medication support
- Nutrition counseling with a registered dietitian
- Psychotherapy and lifestyle change plan
Why Choose Medabolic at RCBM?
- A truly integrated team of psychiatrists, therapists, PAs, and dietitians
- Rooted in 30+ years of clinical experience
- Designed to treat both mind and body
- Ongoing support, not just a one-time consult
Who It's For
- Adults managing chronic weight challenges
- Individuals seeking GLP-1 treatment with proper monitoring
- People whose weight is affected by mental health or medication
- Those who want an alternative to commercial diets or surgery
FAQs
How do I know if this Medabolic program is right for me?
Medabolic is a lifestyle management program using a multi-disciplinary approach through medical nutrition therapy, psychotherapy, and medication management. We use a collaborative method to address the topic of risk factor reduction through weight management that is evidence-based and does not use trendy, unsubstantiated treatments. We approach weight concerns from a risk factor perspective vs aesthetics. In collaboration with your primary care team, we offer the psychological and psychiatric components that are often missing from most programs that address weight management programs. Although they may say they do, they may not be equipped with proper credentialed staffing.
In addition, diagnostic testing determines whether a patient is a fit for our Medabolic Program. If patients are determined to have eating disorders, they will be referred to our eating disorders program at RCBM. The result of our diagnostic testing guides your treatment. Our highly trained team of registered dietitians, psychotherapists, and medication providers integrates a personalized approach based on comprehensive assessments by their respective disciplines.
Share Link: How do I know if this Medabolic program is right for me?
What are the steps to joining the Medabolic program and what should I expect in each appointment?
Upon contacting our office and an initial screening by our Medabolic Intake Coordinator, if appropriate for the program, you will be sent a Medabolic Program Patient Intake Questionnaire to determine further whether you are an appropriate candidate for the program.
If you are an appropriate candidate for the program, you will be scheduled with the following providers who offer the following treatment:
Our registered dietitian (RD) will:
- Conduct a nutrition assessment.
- Collaborate with you to create a personalized nutrition care plan using a weight-inclusive and weight-neutral approach.
- Educate you on nutrition-related potential side effects of GLP-1s if you are prescribed these medications.
- Ensure nutritional adequacy and develop a plan for sustainable progress.
- Review nutrition, behavior, and exercise/movement logs in detail and provide continued support.
- Address behavioral aspects such as emotional eating, mindful eating practices, and fostering a healthier relationship with food and your body.
- Collaborate with your medical provider and therapist to achieve optimal outcomes using a multi-disciplinary and integrative approach.
Your therapist will work with you to:
- Identify triggers to eating behaviors.
- Assess underlying mental health issues contributing to weight concerns.
- Explore maladaptive habits and replace them with positive ones.
- Involve family members, when appropriate, who can help support you as you work toward your goals.
- Help to pave the way for sustained lifestyle changes.
- Understand how your thoughts, feelings, and behaviors intermingle to affect your eating habits.
- Adapt new habits to help increase your willpower, avoid impulsive eating, and avoid triggers.
- Help you gain insight to better manage the stress and anxiety that impedes weight loss progress.
- Address hidden issues holding your progress back.
- Help you learn the root psychological causes of your health struggles.
- Implement small changes to your lifestyle and therefore sustain your weight loss.
Our medical provider will:
- Perform an initial physical through telehealth. Please note that patients on a GLP-1 must be seen at least once per year in person through the CareSynch program and, at that time, have a physical exam through the CareSynch program.
- Order lab work required for the Medabolic program.
- Request diagnostic assessments to ensure accurate diagnosis and treatment of co-occurring mental health conditions.
- After collaborating with the Medabolic multidisciplinary team and reviewing your medical and mental health history, lab work results, and diagnostic assessments, the prescriber will explore medication options.
- Continue to collaborate with your registered dietitian and therapist to achieve optimal outcomes using a multi-disciplinary and integrative approach.
Share Link: What are the steps to joining the Medabolic program and what should I expect in each appointment?
What medications are offered in the Medabolic program?
The medications listed below are offered in the Medabolic program. You can learn more about them in their individual links:
Semaglutides (GLP-1s):
Note: Most health plans stipulate that an effort to change diet and exercise habits must be made before authorizing and re-authorizing coverage for most weight loss medications. Other stipulations apply. Please contact your insurance plan for your plan’s specific criteria.
Share Link: What medications are offered in the Medabolic program?
What are the potential side effects of weight loss medications?
Side effects are common, but they can be well managed with good nutrition practices, which can be personalized based on your experience working with a dietitian.
Please see the following manufacturer’s website for the full side effects of each medication:
Lilly:
Please see this link for a list of full side effects created by the medication manufacturer for Zepbound.
Novo Nordisk:
Please see this link for a list of full side effects created by the medication manufacturer for Wegovy.
Share Link: What are the potential side effects of weight loss medications?
The Sustain Program - Nutrition Curriculum by our Registered Dietititans
The following is what you should expect from your registered dietitian during your medical nutrition therapy sessions:
Whether you're here to explore healthier habits, improve your relationship with food, or manage co-occurring medical and mental health concerns, our dietitians are here to support you every step of the way through a personalized nutrition journey rooted in care, science, and sustainability.
Session 1: Your Nutrition Story
We start with a comprehensive nutrition assessment to understand your full story—not just what you eat but also how you feel about food and your body.
In this session, we’ll explore:
● Your current nutrition concerns and goals
● Past diets or programs that didn’t work for you
● Eating habits and challenges (both past and present)
● Barriers that get in the way of eating well
● How you feel about your body and food
● Your medical and mental health background
Together, we’ll begin setting personalized, realistic goals. Plan for about 60 minutes for this session.
Session 2: Personalized Fuel Plan
Using everything we’ve learned, we’ll design a nutrition plan that actually works for your life. This includes:
● Understanding how carbs, protein, and fat fuel your body
● Building balanced plates that support your goals
○ Tailoring recommendations based on any medical or mental health conditions
○ Guidance for those using medications like GLP-1s
● How to stock your kitchen for success (grocery list tips)
● Food logging options that work for your style
○ Apps
○ Phone notes
○ Food photos
○ Pen and paper
Session 3: Eating with Confidence
We’ll review your food logs and help you refine your daily habits, with support that feels practical and kind - not restrictive.
You’ll learn:
● How to adjust meals for balance and satisfaction
● Simple snack and meal ideas
● Quick recipes and nourishing takeout options
● How to understand hunger and fullness cues
● Tools to prevent emotional eating before it starts
Session 4: Moving with Joy
This session is all about tuning into your body’s needs and making movement something that feels doable and even enjoyable.
Topics include:
● Finding the kind of movement that’s right for you
● Fitting activity into a busy life
● How to fuel your body for different activity levels
● A review of lab results and how they relate to your nutritional needs
Based on when lab work and diagnostic assessment are completed, the dietitian will review results pertaining to nutritional status and nutrition-related co-occurring disorders.
Additional Sessions: Deepen Your Journey
For those continuing with us, we offer ongoing support tailored to your evolving needs. Topics may include:
● Advanced nutrition education (micronutrients, gut health, etc.)
● Meal prep and planning strategies
● Intuitive eating and mindful eating exercises
● Emotional support and body image work
● Accountability tools and progress check-ins
● Turning “I know this” into “I live this”
Share Link: The Sustain Program - Nutrition Curriculum by our Registered Dietititans
How will the Medabolic program set me up for success?
As a medical program, we integrate medication management, psychotherapy, and nutrition counseling into our Medabolic program so that you can achieve the best possible outcome in weight loss and maintenance. One of the most critical lifestyle changes you can make is adjusting your diet, which will significantly impact the sustainability of your weight loss while on the medication and once you discontinue medication and also mitigate side effects when you are on the medication. Additionally, it is essential to address other lifestyle factors, including establishing a healthy relationship with exercise, ensuring adequate sleep, managing stress, and moderating substance use where applicable. Developing a positive relationship with food and your body is also crucial for long-term well-being and weight management.
Share Link: How will the Medabolic program set me up for success?
How fast can I expect to lose weight?
The rate of weight loss achieved with GLP-1 medications varies among individuals and is influenced by lifestyle modifications, including exercise and nutrition. It is critical to avoid excessive weight loss, as rapid loss can result in muscle degradation, nutritional deficiencies, and potential malnutrition. Without GLP-1 medication, a safe and sustainable rate of weight loss is 0.5 to 1 pound per week.
Share Link: How fast can I expect to lose weight?
Is Medabolic only for individuals who want to take medication for weight management?
No. Medabolic can benefit anyone who needs support with weight management. Independent of medication management, this program can help you:
- Implement medical nutrition therapy recommendations to address risk factors.
- Provide tools to address emotional eating and behaviors and end the dieting mentality.
- Help you learn the root psychological causes of your health struggles.
- Evaluate various types of joyful movement that you can implement into your daily routine as a lifelong commitment.
Share Link: Is Medabolic only for individuals who want to take medication for weight management?
How do I get started in the Medabolic program and do I have to be a patient at RCBM to join?
If you are a current patient at RCBM, please contact our office at (248) 608-8800. If you are new to RCBM, please complete our new patient registration form to start the admission process.
Individuals must reside in Michigan and be willing to come to the office if needed.
We look forward to working with you!
Share Link: How do I get started in the Medabolic program and do I have to be a patient at RCBM to join?
Watch: Expert Insights on Weight Management Program

Medabolic Program
Derek Susalla, PA-C discusses the multi-disciplinary weight management program at RCBM.
What is the Medabolic program?
This video illustrates what to expect in the Medabolic program.Meet the Providers Who Offer Care for Weight Management Program
Joel L. Young, MD, Medical Director and Founder
Read More

Ann Dakki, PA-C
Read More

Derek Susalla, PA-C
Read More
Rachel Ford, PA-C
Read More
Beverly Price, RD, MA, CEDS-C, E200-RYT, C-IAYT
Read More
Chelsea Butler, RDN, MSN (formerly Carpentier)
Read More
Jessica Grzybowski, RDN
Read More

Wendy Saal, MA, LPC
Read More
Women’s Mental Health and Wellness

Research consistently shows that women suffer from mental illness at a higher rate than do men. This is likely due to a combination of the unique stresses women face, such as the pressure to conform to an unrealistic beauty standard or to be a perfect mother, along with factors such as hormonal shifts.
We work with women of all ages to combat mental illness and manage challenging mental health symptoms. We understand that mental health concerns—whether they be relationship issues or severe depression—rarely derive from a single cause. Instead, we treat the whole person, examining the complex interplay of biology, life history, environment, nutrition, and many other factors. We partner with you to find solutions, both medical and lifestyle-based, that fit seamlessly into your life and align with your values.
What Challenges Do Women Face?
Women often experience unique mental health challenges tied to hormonal changes, reproductive transitions, and life pressures. RCBM offers care for:
- Postpartum and perinatal depression
- Trauma and PTSD
- Anxiety and chronic stress
- Eating disorders and body image concerns
- Perfectionism and identity challenges
Our Approach to Women’s Mental Health
Our trauma-informed and collaborative care team provides:
- Individual therapy and counseling
- Psychiatric support
- Holistic, whole-person treatment planning
- Compassionate care in a judgment-free space
Why Choose RCBM?
- Female-led clinical teams with expertise in women's mental health
- Experience in reproductive psychiatry, trauma, and identity work
- Supportive environment designed for long-term healing
Services We Offer
- Therapy for trauma, anxiety, and depression
- Eating disorder support
- Couples counseling
- Medication evaluation and management
- Group therapy for life transitions
What to Expect
- Initial intake with a trained clinician
- Matching with a therapist or psychiatrist
- Collaborative care plan creation
- Ongoing sessions tailored to evolving needs
FAQs
Infertility and Pregnancy Loss
Though both men and women often aspire to be parents, women are taught from an early age that motherhood is a special, and perhaps mandatory. For this reason, infertility can directly affect a woman's self-esteem and overall mental health. Moreover, the complex biological changes associated with treating infertility can wreak havoc on a woman's hormones, making an already difficult time even more stressful.
Women who struggle with pregnancy loss are often hesitant to seek help. There is still the stigma associated with miscarriage, and well-meaning loved ones may inadvertently say hurtful statements. Your partner might not feel as connected to the baby like you, and the sudden hormonal shift associated with a pregnancy loss can compound these challenges. We work with women to navigate the pain associated with infertility and pregnancy loss, to talk to their partners about their pain, to regain a sense of identity after pregnancy loss, and to move forward with confidence regardless of the outcome of fertility treatments.
Share Link: Infertility and Pregnancy Loss
Eating Disorders and Body Image Concerns
Eating disorders are a serious mental health condition. The cause of eating disorders is multifactorial, with women making up 75% of those diagnosed with eating disorders. Eating disorders include, but are not limited to, anorexia nervosa, bulimia nervosa, binge eating disorder, and other specified eating disorders. We have a comprehensive and skilled eating disorders team that can treat these issues.
Outside of eating disorders, some women have trouble achieving their usual weight post partum or struggle with obesity. For those patients who have underlying risk factors and do not have an active or history of an eating disorder, we can work with you to achieve a healthy weight without the use of diets or "gimmicks."
Share Link: Eating Disorders and Body Image Concerns
Trauma and Abuse
Trauma is a common experience among women. As many as one in four women have been raped, while one in three has experienced violence by an intimate. This type of interpersonal trauma can have far-reaching effects on your self-esteem, relationships, and sense of safety. Women who have experienced trauma may develop symptoms of post-traumatic stress disorder (PTSD) or adopt unhealthy coping mechanisms, such as alcohol use or refusing to leave the house.
We work with you to help you understand how your trauma has affected your life and sense of self. We never push you to talk about something you are not ready to address. Instead, we move slowly and deliberately, helping you feel safe to discuss the pain you have faced.
Share Link: Trauma and Abuse
Premenstrual Dysphoric Disorder (PMDD)
Diagnosis and Symptoms: Premenstrual Dysphoric Disorder (PMDD) is characterized by specific symptoms that must be present in the 7 to 14 days before the onset of menses, and start to improve within a few days after menses begins. Symptoms can become minimal or absent in the week post-menses and across the majority of menstrual cycles. According to the DSM-5 criteria, at least five symptoms must be present. These symptoms must include one or more from a core set of affective symptoms: marked affective lability (e.g., mood swings, increased sensitivity to rejection), marked irritability or anger, markedly depressed mood/hopelessness, or marked anxiety/tension. The remaining symptoms can include: decreased interest in usual activities, subjective difficulty in concentration, lethargy, marked change in appetite/overeating/cravings, hypersomnia or insomnia, a sense of being overwhelmed or out of control, and physical symptoms like breast tenderness or bloating. The symptoms must also be associated with clinically significant distress or interference with life activities.
Testing and Risk: There are no lab tests to confirm PMDD symptoms. The only type of "test" involves two months of consecutive symptom collection using prospective daily ratings. PMDD occurs during the Luteal Phase (7 to 14 days before bleeding) of the menstrual cycle. Individuals assigned female at birth and of childbearing age are at risk, as well as those with a family history of PMDD, Postpartum depression, or mood disorders. PMDD is separated from PMS because PMDD is more of a behavioral disturbance, while PMS is a broader term for behavioral change.
Management: Treatment options for PMDD include both pharmacological and nonpharmacological approaches. Selective serotonin reuptake inhibitors (SSRIs) are a first-line treatment for severe symptoms of PMDD, and oral contraceptives like Yaz are also effective. Nonpharmacological ways to help include cognitive behavioral therapy (CBT), yoga, acupuncture, and supplementation with Calcium, Magnesium, or Vitamin D (based on lab work and consultation with your provider). However, there is controversy and inconsistent data regarding nonpharmacological recommendations.
Share Link: Premenstrual Dysphoric Disorder (PMDD)
Prenatal and Postpartum Depression
Pregnancy is a life-altering event that spurs a whirlwind of changes in your body—weight gain, unusual medical symptoms such as swelling and high blood pressure, along with a sense that your body is no longer fully your own. It's no wonder that so many women experience depression either during or immediately after pregnancy.
Although not the sole culprit, hormonal shifts play a significant role in pregnancy-related mental health issues. Women are more vulnerable to pregnancy-related mental illness if they feel unsupported, have a history of trauma, struggle with financial issues, experience health problems during or after pregnancy, or do not receive adequate assistance to tend to their own health.
We work with you to tease apart the various causes of your depression. We don't dismiss you as just another case of hormones gone awry. Instead, we'll craft a comprehensive plan to help you get back to being yourself, so you can enjoy motherhood and find a sense of meaning in bonding with your baby.
Share Link: Prenatal and Postpartum Depression
Transitioning Into Motherhood
There is perhaps no more profound life change than the transition to motherhood. Suddenly, you are responsible for caring for a small person. Many women find that the burdens of motherhood fall primarily to them, based on generations of gender norms. Additionally, women without partners may feel completely alone. From navigating breastfeeding to coping with the stress of a screaming infant, while managing the mixed emotions of transitioning back to work, to rediscovering who you are separate from your identity as a parent, we can help you make a smooth transition to motherhood.
Share Link: Transitioning Into Motherhood
Relationship Issues
From an early age, women are taught to prize their relationships. Relationships make us human, enrich our lives, and offer support through the challenges of life. Too often, though, relationships themselves become the source of life's worst challenges. Infidelity, divorce, breakups, abuse, and relationship conflicts can overwhelm even the strongest women, leaving them wondering how to cope.
We will work with you and your partner to get your relationship back on track. Even if your relationship is ending or your partner is unwilling to seek counseling, we can help. Therapy sessions can offer clarity, a renewed sense of hope, and a deeper faith in your ability to resolve the problems in your relationship—or to move onto a more positive relationship.
Share Link: Relationship Issues
Watch: Expert Insights on Women’s Mental Health and Wellness

Nutrition Concerns for Women Over 50 | with Beverly Price
Rochester Center for Behavioral Medicine’s Beverly Price, a Certified Eating Disorders Registered Dietitian, joins us to discuss 'Nutrition Related Concerns for Women Over 50'. Learn about triggers for eating disorders, heart disease, weight control and management, exercise, and helpful solutions to a journey of a more healthy lifestyle.
Couples Counseling
Marni Stone, LMSW, is a graduate of the Couples Institute. In this video, she discusses how she can help couples and families with communication skills, coping techniques, patterns of interaction, and other important areas of stress.
Hear from Dr. Hutton
Sarah Hutton, MD, RCBM's Associate Medical Director, specializes in women's health, which includes pre-menstrual dysphoric disorder, peri and post-partum depression, and issues surrounding menopause.
What is Premenstrual Dysphoric Disorder (PMDD)?
Elizabeth Sweet, DNP, APRN, PMHNP-BC discusses PMDD, which is a severe form of premenstrual syndrome (PMS) that causes intense emotional and physical symptoms, such as extreme mood swings, anxiety, and depression, in the week or two before menstruation. These symptoms can significantly disrupt daily life and relationships. Lizz also discusses treatment options.
Women and Trauma
Melissa Oleshansky, PhD discusses how she works with women recovering trauma, including CBT, trauma-focused or gentle-body based therapy. Dr. Oleshansky also recommends daily health habits to reduce stress and walks you through deep breathing and grounding exercises.Meet the Providers Who Offer Care for Women’s Mental Health and Wellness
Sarah Hutton, MD, Associate Medical Director
Read More
Aundreah Walenski, LMSW
Read More
Elizabeth Sweet, DNP, APRN, PMHNP-BC
Read More

Erika Samulak, MA, LPC
Read More
Judith C. Redmond, LPC, LLP, CAADC
Read More

Kasey Downing, LLMSW
Read More
Marni Stone, LMSW
Read More
Sydney Salloum, LPC
Read More

Tracy Weitzman, MA, LLP
Read More
Wendy Saal, MA, LPC
Read More
Related Titles from the RCBM Reading and App list:
And Now We Have Everything: On Motherhood Before I was Ready - By Maeghan O'ConnellAnxiety, Worry, Panic Attacks, Obsessions and Compulsions - By Pamela Wiegartz and Kevin Gyoerkoe
The Pregnancy and Postpartum Anxiety Workbook: Practical Skills to Help You Overcome Anxiety, Worry, Panic Attacks, Obsessions, and Compulsions - By Pamela S. Wiegartz and Kevin L. Gyoerkoe
Me v PMDD - PMDD Tracking App











